- This topic has 39,835 replies, 1,030 voices, and was last updated 2 weeks ago by Klunk.
-
The Coronavirus Discussion Thread.
-
curlywhirlyFree MemberPosted 3 years ago
Yeah, you stick it to The Man just to prove a point to yourself.
I think you have missed my point entirely. Nothing to do with sticking it to anyone. But if people feel pushed or coerced into something by others, rather than letting them decide what is best for themselves based on an open and honest appraisal of the data, and taking into account their personal circumstances, then I think we have a problem.
PoopscoopFull MemberPosted 3 years ago@ CountZero
I’ve only been dipping a toe into the thread recently as I’m “content” with the info I have from here for a bit, until I need more info/guidance.Hence I’ve only just read the dreadful news. Genuine and heart felt condolences CZ.
TiRedFull MemberPosted 3 years agoSorry but whatever your beef is with someone, that someone is not me.
Welcome to the forum and the debate. Your comment about 0.3% mutation is sadly not really relevant. The spike protein, which is subject to significant immune (and now vaccine) selection pressure, has recorded mutations at more than 500 sites thus far (GISAID database). That some of those confer additional transmissibility has been noted (N501Y), and perhaps additional morbidity (E484K) is interesting. Vaccine studies against the latter strain has shown a degree of escape with low protection against symptoms (better against more serious disease). It’s still VERY early to see evolution to benign viral strains.
As for herd immunity – well I am afraid that there are four other endemic coronaviruses that would refute the notion of population protection. Waning immunity and seasonality drives annual outbreaks of these (two account for about 18% of common colds). SARS-CoV-2 is unlikely to be very different. It’s not going to go away.
I share your sentiment on providing NHS treatment, but when half of beds have been taken by COVID patients (who have immediate hypoxic needs), the NHS will struggle with routine care provision. That is why we have had three months of Stay At Home provision. Whether one agrees with this policy or not, the outcome (together with rising immunity and vaccination) has been a 95% reduction in COVID transmission pressure. Vaccination is the means of preventing the resurgence. At the moment the evidence (mainly from Israel) suggests that this is a prudent approach. We will see.
EdukatorFree MemberPosted 3 years agobut did Madame make use of oral contraceptive earlier on in life?
That’s a very good example of risk assesment. When young and in a low risk category she did, however at age 32 we reverted to condoms. I should have bought shares in the LRC at that point. When young the risks associated with (perhaps unwanted) pregnancy are higher than taking the pill, as women get older the balance tips to using condoms with a slightly higher risk of unwanted pregnancy but lower risk of thrombosis or other side effects, so we did.
nickcFull MemberPosted 3 years agorather than letting them decide what is best for themselves based on an open and honest appraisal of the data, and taking into account their personal circumstances, then I think we have a problem
As long as your individual assessment takes into account the people around you and your responsibilities towards the greater community, then I’ve got no problem with your statement.
@CountZero , like others on this thread I’ve just stumbled across your terrible news. I don’t know how to express myself other than to say you have my deepest condolences & sympathies.theotherjonvFull MemberPosted 3 years agoI should have bought shares in the LRC at that point.
Humblebrag.
My major concern at that time was them going out of date……
willardFull MemberPosted 3 years ago@CountZero There are no words that I can say that can ease what you must be feeling. My deepest condolences.
joepudFree MemberPosted 3 years agoI don’t want people to be forced to take a vaccine against their will. I would like everyone who can get a vaccine to do so, including those at low risk of COVID related complications, to help protect the population as a whole. I don’t think this is a controversial opinion.
Its not a controversial opinion. But I guess the question is if you yourself are at a lower or no risk what so ever, you can’t bemoan those who are at a higher for not wanting to take that risk. As a fit 35 yr old am I concerned about the oxford jab, yes especially when some countries are saying anyone under 55 or something shouldn’t take the Oxford jab. I really hope when my turn to get a jab finally comes I get offered something else I don’t particularly want the oxford one now given recent news.
kelvinFull MemberPosted 3 years agoTransparency and accountability…
The FPA has formally complained to the @DHSCgovuk
for the unacceptable treatment reserved to foreign journalists who are trying to cover the *global* pandemic. Barring access to news sources is never a good way to promote "Global Britain" and is an infringement of #mediafreedom pic.twitter.com/kT1N4iPBt4— Foreign Press Association in London (@FPALondon) April 8, 2021
DelFull MemberPosted 3 years agoEd, risk of thrombosis from oral contraceptive was put at ‘between 600 and 1400 per million’ last night by an interviewee on PM Vs 4 per million for AZ.
Madame’s choice of course.
EdukatorFree MemberPosted 3 years agoFunny how they bump up the numbers for the contraceptive pill when it suits them. I don’t know where the interviewee got their numbers from but that range is much higher than quoted elsewhere, for example:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3626808/
That’s on a per year basis. Madame is calculating on having to wait a few weeks for an alternative vaccine, maybe, all the current dates in our area are Pfizer and Moderna. The risk of waiting an extra three weeks for someone who has no risk factors for Covid and we think got through it March 2020 with a sore throat, shivers, tiredness, conjunctivitis and Covid toes seems more acceptable than AZ aged under 60.
MoreCashThanDashFull MemberPosted 3 years agoAs a fit 35 yr old am I concerned about the oxford jab, yes
Concern is perfectly valid.
But hopefully you are more concerned about being badly hurt or killed in a car accident, or struck by lightning*, or any of the other unpleasant things more likely to happen to you than to have a blood clot after having the vaccine.
*I’ve not double checked the lightning data, may not be accurate comparison
amodicumofgnarFull MemberPosted 3 years agoCountZero – really sad to read about your loss, deepest condolences.
chrispoFree MemberPosted 3 years agoWhat’s making people look silly?
Their arrogance.
Those who saw fit to belittle anyone who had doubts or questions about whether the vaccine’s short test period was enough to pick up possible side-effects are looking a little silly now that this new side-effect is emerging.
Others who were more measured will continue to attract respect.
kelvinFull MemberPosted 3 years agoYou were talking about someone who refused all vaccines, yes? Were they passing on that risk to children as well? Remind us…
kelvinFull MemberPosted 3 years agoIs it not what you were talking about when others replied in a way that you say was not measured enough?
ferralsFree MemberPosted 3 years ago@Del – is that supposed to be a link? It’s just coming up as a number on my phone
kelvinFull MemberPosted 3 years agoThe link is just your phone being clever and turning it into a dialling link. It’s not a URL in the post.
theotherjonvFull MemberPosted 3 years agoI am not disputing that you expressed concern that turns out to have been correct. I’m still not sure it wasn’t a guess, or even taking an opposite view for the purposes of argument, but that’s something I have to wrestle with, I don’t have data to justify it so it is not an accusation.
If the virus hadn’t been rolled out as widely as it has been, these side effects would not have been seen. In the meantime, many lives have been saved / are being saved by it. A normal sized trial only picks up common side effects, and would have left us months behind where we are now.
It’s normal that things come to light as the population usage increases, that’s exactly why there is the ‘yellow card’ scheme for reporting previously unknown side effects. That new side effects are coming to light is no evidence of anything being rushed / corners cut / some marvellous pharma conspiracy. Now we know they exist, we replot the course. That’s how it works.
meftyFree MemberPosted 3 years agoAm I reading that incorrectly?
Same way as me, essentially the same order of magnitude.
theotherjonvFull MemberPosted 3 years agosame as me I think
“5-10 per 10,000 womanyears
so that means if 10,000 women took the pill for a year there would be 5-10 clots.
I suppose you could say that’s 10,000 x 365 exposure = 3.65 million so (top end) 10/3.65M is 1/365,000 so the chance of getting a thrombosis on any particular exposure is substantially less than the chance of getting a clot due to the (one) exposure to the vaccine.
But if a woman’s on the pill for 10 years, that increases the number by 3650x
Or – on a yearly basis (hypothesis, annual vaccination needed) – 365x higher
grahamt1980Full MemberPosted 3 years agoBeen taking a break from the thread as the az stuff is getting to me.
But CZ my heart goes out to you. So sorry for your loss.
You could not have done anymore than you did, hindsight is always one of those things, i just hope that others will now be saved from knowing what to do. None of that eases your loss. As ever the forum will be here for youEdukatorFree MemberPosted 3 years agoYes, 500-1000 overall, Del and theotherjonv.
However in younger women it’s 400-500, that’s the at risk age group with AZ and a low risk category for Covid itself. As TiRed alluded, at some age the increased risk from vaccination and decreasing risk from the disease itself makes vaccination questionable ethically – especially when alternative lower risk vaccines exist, and they do.I think the Germans have it right, AZ for the over 60s. And I’m over 60, and male so I’ll play the statistical game if I’m offered AZ – with the local equivalent of a do not resucitate letter valid for a month after being vaccinated. No smiley.
Incidentally I was on the phone with my Doc recently, he’s been getting feedback/results on AZ. Apparently the immune system response to AZ is **** enormous with remarkable antibody production – he has no doubt about the efficacity. The response is also fast, within a couple of weeks.
theotherjonvFull MemberPosted 3 years agooh, I absolutely agree that if there’s an alternative then we should use it. But if there was no alternative, and the choice was AZ vs Covid – comes back to what I said this morning, that the general public does not have a good grasp of risk and risk-benefit.
tpbikerFree MemberPosted 3 years agowas enough to pick up possible side-effects are looking a little silly now that this new side-effect is emerging
They aren’t really though are they. Everyone with an ounce of common sense knows that some serious side effects may happen, but they would be very very rare. Which they are.
If this vaccine had been tested over the usual period would they have picked it up given they would need 1m test vaccinations for every 4 clotting cases? It seems highly unlikely.
Fact remains this vaccine is safe for practically every one who takes it. It’s maybe not quite as safe as the pfizor vaccine but don’t try and make out that only enlightend people like yourself called out that this incredibly rare issue might occur.
That said being exceptionally rare doesn’t make it any less tragic for those people it does happen to. Thoughts are with CZ at this time.
EdukatorFree MemberPosted 3 years agoComparisons with the contraceptive pill become unfairer the deeper I dig:
chrispoFree MemberPosted 3 years agodon’t try and make out that only enlightend people like yourself called out that this incredibly rare issue might occur.
Absolutely not. Sarcasm noted though. That has been my problem all along. I’m a scientist* and you’re not, so I will play the man not the ball.
*Not all the scientists on here, I hasten to add.
Theothertjonv: I agree entirely. It’s always been the behaviour on here from some that I have a problem with, not the vaccine. I had some doubts about the vaccine, yes, but did some research, listened to people who seemed worth listening to*, and decided I should have it to do my bit, especially after the virus killed my best friend. I wasn’t able to convince the ex, but that was always a long shot.
*Including a couple on here. Thank you.
CountZero: I’m sorry for your loss.
TiRedFull MemberPosted 3 years agoThere are multiple genetic mutations that can lead to coagulation disorders. One of the most well-known is Factor V Leiden. Sadly one test for this is a pulmonary thrombosis rapidly after initiating oral contraception. My cousin is homozygous and you can guess how we know this. She almost died but for her GP. My mother was heterozygous. My wife has another Leiden mutation that is rarer but has the same issue and she cannot take OC. She’s heterozygous and that was discovered after a clot (unrelated to OC). I’ve been tested and don’t carry any Leiden mutations, so children are in the clear from at one side and 50% chance of both – hence my test.
Rare events may later come to be understood by underlying biology. Sadly this is often the way biology reveals itself. We have much to learn, but the pharmacovigilence of process is working as intended.
EdukatorFree MemberPosted 3 years agoIf this vaccine had been tested over the usual period would they have picked it up given they would need 1m test vaccinations for every 4 clotting cases?
The British figures are lower than quoted elsewhere.
12 cases from the first 2 million doses in France and 31 from 2.7 million in Germany:
Bei 2,7 Millionen verabreichten Erstdosen und 767 Zweitdosen von AstraZeneca sind nach aktuellem Stand des Impfmonitorings des Robert-Koch-Instituts (RKI) 31 Fälle von sogenannten Sinusvenenthrombosen aufgetreten.
Vaccination strategies changed in both countries as a result with AZ for over 55s in France and over 60s in Germany. Edit: the cases disproportionately hit medical and care home workers who were the first young people to be given AZ. The overall figures don’t look to bad but when you separate the medical workers from the oldies who’d also been given AZ the problem was highly visible and clearly demonstrated the threat to younger people and especailly women.
theotherjonvFull MemberPosted 3 years agoBut 4/million, 6/million and even 11.5/million – they’re broadly the same number.
It’s not like anywhere else is reporting 100/M or 1000/M
I did wonder initially if it could even be batch or plant specific, but that seems to be off the table now.
EdukatorFree MemberPosted 3 years ago2 cases from a few hundred staff in one hospital was the wake up call. In young women ” 100/M” is plausible. You’ll find out when/if AZ is used to vaccinate 30-year-old women. It would be unwise IMO. In Nancy CHU vaccination was stopped until Pfizer was available.
theotherjonvFull MemberPosted 3 years agoyes, that’s also what the data is starting to reveal…. this is increasingly age and possibly gender specific
singletrackmindFull MemberPosted 3 years agoIn england, are we allowed family sleepovers at the moment?
My nasty neighbour has his son staying tonight. Just another reason to dislike himIs thrombosis via Az more common than dvt after a long haul flight? So are you stopping all flights over say 8hrs as the dvt risk is real then. Just a thoght.
mytiFree MemberPosted 3 years agoThanks for that edukator. As a fit, healthy, low covid risk 39 year old taking oc for medical reasons I’m currently weighing up the risk/benefits. I’m thinking by the time im offered a jab it may well have changed to avoid az anyway but we’ll see.
mudmuncherFull MemberPosted 3 years agoIt seems the younger you are the stronger the immune reaction you have to the jab which possibly explains the greater prevalence of clotting events with decreasing age. That being the case I wonder if that could be mitigated by reducing the vaccine dose for younger people? That would also help to solve the vaccine shortages, e.g. if we gave 1/2 dose for under 50’s that may still give a sufficient immune response for protection with less side effects and mean we could jab the under 50’s in half the time.
curlywhirlyFree MemberPosted 3 years agoThat is why we have had three months of Stay At Home provision. Whether one agrees with this policy or not, the outcome (together with rising immunity and vaccination) has been a 95% reduction in COVID transmission pressure.
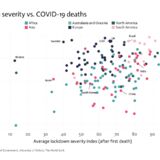
This is the bit I just can’t get my head around. People are claiming that lockdown is the answer to reduce deaths when all the data from around the world show no correlation between lockdown stringency and Covid-19 mortality as can be seen from the plot here:

Also we were told that keeping schools shut was essential to keep cases down, and SAGE modelled the return of school kids as having a big impact, partly because school children were not vaccinated. Yet schools have gone back and the surge of infections has not happened. Is it possible that SAGE have got their assumptions as to what measures work or not wrong in their modelling because the data on the ground does not seem to support it?
EdukatorFree MemberPosted 3 years agoI agree, Mudmuncher. Vaccines like other medication tend to be one size fits all. Whether you’re a 45kg female or 100kg+ male they put the same amount in your arm. Age 30 or 80, same dose. I hadn’t thought about it from the shortage point of view but you’re right, the vaccination could potentially be achieved faster.
After experimenting with my asthma meds I’ve found a child’s dose suits me better, same benefit, less side effects. I’m 64kg BTW. There must be an optimum vaccine dose for each personal profile, I hope they are working on it.
You must be logged in to reply to this topic.