I agree. Even though I support what we did, I think we had tough choices and while we did mainly the right things, doesn’t mean we did them in a timely way, or effectively. We need to review and reflect and think whether we got it right, and what we have learned from it.
Nicely put.
I understand the calls for a lockdown when Omicron kicked off, as we didn't have data on the severity and our previous attempts at lockdown had been late. With perfect hindsight and what we know now, I think locking down may have been an overreaction, it's not been as severe as it could have been, but my view on the deaths from this wave will be different to most other people's views.
The government got lucky this time with not locking down. And maybe other actions short of lockdown might have still been appropriate.
Thanks @barrysh1tpeas @kelvin @MoreCashThanDash and @theotherjonv
good to get some opinions. Will mull it over a bit
Now for some optimism about the next pandemic sarbecovirus. This article is a little technical but explains the history of the development of Paxlovid. The data is published in a Science paper here. But the real reason to have some optimism is Fig 5d which I have reproduced below.
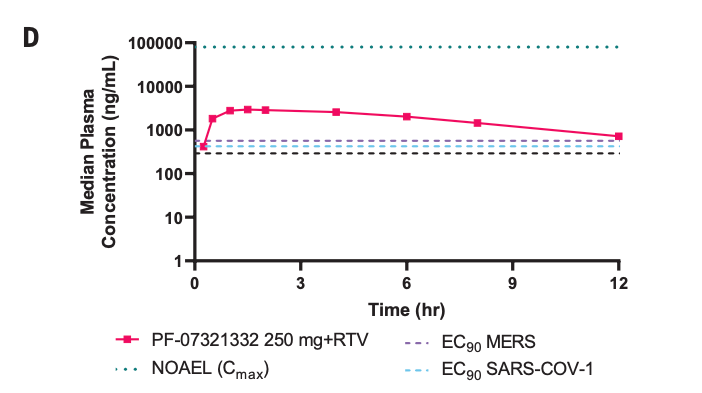
Why optimism? Well, the red line is the drug concentration in humans during the 12-hours between doses. The dashed lines are the target levels for SARS-CoV-2 AND SARS-CoV-1 and importantly MERS. Paxlovid is capable of inhibiting all past SARS-inducing coronaviruses. Now the TOP dashed line, NOAEL*(Cmax), is the toxicity limits for the drug. So when the next virus comes along, either the drug will work, or the dose can be raised until it is likely to work. That was NOT the case for all previous antivirals against SARS-CoV-2. This new drug is the first approved against what looks like an excellent new antiviral target (for this and other viruses).
*NOAEL is "No observable adverse effect level" in preclinical toxicity testing.
Akbar seems to asking perfectly sensible questions which I would hope any inquiry addresses as we need to learn whatever lessons we can. It seems that a shielding approach could have been more effective but whether it would have been realistic to come to this conclusion early in a pandemic when you don't know which age group are being hit hardest is another matter. Allowing covid to spread into the care sector seems to be a common fault made by most of countries that had bad first phases relatively and that it will be interesting to see who drove the decision to transfer patients in the UK.
Now we are reliant on vaccines, the only reason to have any restrictions is if we are in danger of having excess deaths due to shortage of NHS capacity so as cases are falling it is right to open up and live a normal life which I certainly will be doing. We certainly can't restrict lives because of long covid.
@TiRed - that is good news. How long until this drug is available for use?
Already approved and purchased by HMG. Manufacture and supply by Pfizer is being ramped up in France for European supply.
https://www.gov.uk/government/news/oral-covid-19-antiviral-paxlovid-approved-by-uk-regulator
Apologies for the link, but the "FINALLY" makes me laugh. it's normally a full year to approve a new drug. Pfizer submitted Paxlovid for review in mid-November!
https://www.****/news/article-10358809/Britain-FINALLY-approves-Pfizers-life-saving-Covid-pill.html
Apologies for the link, but the “FINALLY” makes me laugh. it’s normally a full year to approve a new drug.
Does mean it was rushed out, untested and an experimental vaccine? Asking for a deluded friend.
😀
No. It was subject to a rolling submission as the data was fed into agencies as soon as it became available. So manufacturing (CMC), preclinical safety, then first human data and finally efficacy and safety. Rather than submitting a massive tome at the end. Also being a small molecule rather than an antibody, drug is gone in a day (rather than a year and a half for AZ's Evusheld). Faster without the ritonavir boosting.
And you are of course welcome to read the EMA assessment report here. MHRA processes for publishing assessment reports seem to be a "work in progress". You can read the summary of product characteristics (SMPC) but that's not the review.
As amazing as that drug sounds how well will it do when people are administered it after say 10-14 days+? Getting it into people a few days after their positive test/symptoms start is not going to happen very often unless we’re all sent a box of ‘em with our positive test results?
It seems that a shielding approach could have been more effective but whether it would have been realistic to come to this conclusion early in a pandemic when you don’t know which age group are being hit hardest is another matter.
We did use a shielding approach. Oh... do you mean "just" a shielding approach? With all us fit, young and able people (with all our fit, young and able coworkers, and fit, young and able families, and fit, young and able customers/clients) not having to reduce our contacts and take other measures to reduce transmission to buy time for vaccines, treatments and knowledge to be made ready?
how well will it do when people are administered it after say 10-14 days+?
Most people who suffer serious morbidity are already in hospital at this point. Needs to be dosed within about 5 days of symptom onset. Three days is even better. Recall Swine Flu, 2009. We had rapid access to Tamiflu via pharmacies. This will come in time for orals.
Akbar seems to asking perfectly sensible questions
they're learning. interspersing reasonable questions gives an air of credibility...
438 deaths recorded in a day. At this late stage of the pandemic, when we have so many tools and so much knowledge available to us.
The highest day for deaths in the last month for England was January 9 when 244 died.
So far. Lots of reporting to filter through there (assuming you are looking at date of death, not date reported). If you are insinuating that we may have already passed the peak for deaths in England, I think (and of course hope) that you are correct. By we won’t know for a while. Nothing can be done about this now anyway, these were all baked in a while back. Admissions are staying stubbornly high though… suggesting death data will also have a longer slower tailing off than case data.
Mrs Onewheel works in a primary school. Over the weekend they had 11 children and one staff member report positive.
And as of this evening, 60 children are off school, having tested positive. 16% of the school.
Come on kelvin, you know better than that. Look at the 7 day average, the last two days were in the 80s due to weekend figures.
Yes it's too high, but I think you've taken it out of context.
There are always two low days of reporting. Every week. I haven’t taken anything out of context, and I agree that date of reporting and date of death are different things, and despite this high reporting figure (highest since last Feb) we are very likely already past the peak day of deaths this winter.
But until deaths are reported, we can’t comment on them.
Last 7 days
1,904
⬆️ 244(14.7%)
We can look at the 7 day reporting, but it still doesn’t give the full picture. I suspect when we look back and have full data that deaths were already falling slowly (or at least have plateaued) before today. At least I hope so.
But commenting on deaths as they are announced, and wishing there were fewer, doesn’t seem out of order.
But until deaths are reported, we can’t comment on them.
Then don't, strangely you chose last Wednesday to quote the death figure too despite anyone who has taken a cursory interest in Covid info - and it seems a full time job for you - knows Tuesdays and Wednesdays are the highest days so care should be taken when quoting then - only a bad faith poster would do otherwise, which makes you rather a big hypocrite. IGNORE.
A question i've been pondering is how exactly are new variants of the virus identified?
I can't imaging path labs are able to analyse each and every sample they come across... so is it a case of healthcare workers noting when symptoms seem different and then following up, or noticing changes in characteristics of spread? (IIRC that's what happened with Omnicron).
Or is there a more formalised methodology being used internationally?
My understanding is that a proportion of PCR tests are checked to see which variant they are or if they are a new variant?
The fraction sent for genotyping varies depending on number of tests. Fewer cases mean a higher proportion are tested. It’s typically about a quarter of all tests. These genotypes are uploaded to GISAID and we lead the world in this. Variants may also be isolated from other countries and tagged by UKHSA via surveillance in GISAID.
That's interesting, thanks, and quite reassuring.
Just about to take Batfink Jnr (5yrs) for her first Jab.
It's at the main Sydney vaccination hub, so it should go smoothly, and by all accounts they've made a bit of an effort for the kids in terms of materials/distractions etc
Lets see how we go, based on previous vaccinations (albeit a year ago) response could be anywhere from "this is fine.... can we go for ice cream now?", to full-on wailing/howling, rolling on the floor, with me having to hold her down.
I have one fun-size packet of Maltesers, one of M&Ms and a Freddo..... hopefully she won't burn through all of that.
Why would you take your 5yr old for a jab?
Really, why?
Yeah, what's this crazy idea about giving children vaccinations?
Why wouldn't you?
Good luck batfink ... i'm sure it'll be fine.
I'm sitting 20 metres away from a large queue of kids doing exactly that.
My kids have been jabbed in accordance with mainstream vaccination regulations as I was, and will be getting their COVID jabs in the next few days.
They both understand the concept that it will reduce the risk of them passing the virus to more vulnerable members of the population.
Kids aren't at risk - especially from Omicron
Myocarditis is real
The bloody jab only works for a few weeks anyway
And give over, you can still pass it on
Jesus, you really have sucked it all up. Give me strength
My kids have been jabbed in accordance with mainstream vaccination regulations as I was, and will be getting their COVID jabs in the next few days.
What actually does this sentence mean - read it back and actually take in what you are saying?
Good god
The bloody jab only works for a few weeks anyway
Whilst omicron is a challenge due to immune escape, estimates of protection from serious morbidity are more than a few weeks. In truth, had we only had the current vaccines and omicron, they’d still be approvable. The fact the mRNA vaccines were so efficacious against the Wuhan strain is what still makes them useful today.
Myocarditis is real
I think we’ve found a Joe Rogan disciple
Whilst omicron is a challenge due to immune escape, estimates of protection from serious morbidity are more than a few weeks
Maybe - and I take specifically your information with due respect.
I'll stand by my judgement that 5yr olds do not need and should not be administered a short term vax that has been proven to have adverse health detriments and will require repeated doses to provide efficacy
My daughter was given her MMR without any hesitation btw
I think we’ve found a Joe Rogan disciple
So, is it not real?
and I take specifically your information with due respect
But you’re not willing to consider those setting vaccination policy in Australia as regards 5-12 year olds have access to and understood good information? It’s not just Australia either, check vaccination rates for the under 12s in the USA, they’re well ahead.
I figure you are referring to the preprint study of Vaers data so no, it is not real.
Damn, If only I previously knew how easy it is to grift a plausible narrative for susceptible minds I could have made a fortune from patreon
What actually does this sentence mean – read it back and actually take in what you are saying?
Erm ... it makes more sense than...
Myocarditis is real
But let's look closer.
1 in 10,000 for adolescent boys...Australian data. About the equivalent of dying in a canoeing accident or skydiving. Both things i would be happy to let my lads do.
I think i've worked out what you were trying to say.
Myocarditis is really unlikely
Or as Mohanna K, Chambers R. Risk matters in healthcare: communicating, explaining and managing risk. Radcliffe Medical Press, Abingdon, UK; 2001 call it Very low.
I’ll stand by my judgement that 5yr olds do not need and should not be administered a short term vax that has been proven to have adverse health detriments and will require repeated doses to provide efficacy
Ok. Stand by it. But why does your judgement have any sway whatsoever? I'll stand by my judgement that flares only look nice if they're made from purple material. I don't care if you wear flares at all.
But you’re not willing to consider those setting vaccination policy in Australia as regards 5-12 year olds have access to and understood good information? It’s not just Australia either, check vaccination rates for the under 12s in the USA, they’re well ahead.
If you haven't worked out that Oz has gone batshit mental, then you are probably batshit mental too.
Kids don't need this vax
I figure you are referring to the preprint study of Vaers data so no, it is not real.
Damn, If only I previously knew how easy it is to grift a plausible narrative for susceptible minds I could have made a fortune from patreon
Myocarditis isn't real? OK, believe that, I'll believe it is
But let’s look closer.
1 in 10,000 for adolescent boys…Australian data. About the equivalent of dying in a canoeing accident or skydiving. Both things i would be happy to let my lads do.
I think i’ve worked out what you were trying to say.
It almost looks like you're quoting figures for actually dying from covid....
Ok. Stand by it. But why does your judgement have any sway whatsoever? I’ll stand by my judgement that flares only look nice if they’re made from purple material. I don’t care if you wear flares at all.
My judgement has no sway
I can judge peoples reaction to events and give my opinion at will. As can you. Who is right, who is wrong?
If you haven’t worked out that Oz has gone batshit mental, then you are probably batshit mental too.
What have they had? 3000 deaths? I’m sure they’ve made loads of mistakes, got things wrong, argued amongst themselves, which country hasn’t? But, I’m not sure we should be throwing stones from the UK.
Batshit mental ... oh, yeah, i'd much rather be living in the UK right now.
Please explain.
What have they had? 3000 deaths? I’m sure they’ve made loads of mistakes, got things wrong, argued amongst themselves, which country hasn’t? But, I’m not sure we should be throwing stones from the UK.
Death rate of 107:1m versus 2,229:1m in the UK.
reeksy
Free Member
What have they had? 3000 deaths? I’m sure they’ve made loads of mistakes, got things wrong, argued amongst themselves, which country hasn’t? But, I’m not sure we should be throwing stones from the UK.Death rate of 107:1m versus 2,229:1m in the UK.
Will be interesting to see how that looks in 6 months tbh, now that they have opened up. I'd have a guess that it will be definitive proof of vaccine efficacy, not that we need it mind, but it'll still be interesting to see how them opening up and letting the virus in affects their numbers over the long term.
Myocarditis isn’t real? OK, believe that, I’ll believe it is
It’s a genuine condition, the scientific community have examined the data with regard to myocarditis rates in unvaccinated vs vaccinated children and come to an entirely different conclusion as to your beliefs regarding risks, perhaps you should choose better gurus to follow, or move to Texas where you’ll fit right in.
I can judge peoples reaction to events and give my opinion at will. As can you. Who is right, who is wrong?
You can give an ill informed opinion all you want, and as for “who is right, who is wrong?”
Doesn’t really need answering does it?
If you haven’t worked out that Oz has gone batshit mental, then you are probably batshit mental too.
Man, you've said some amazing stuff in this thread but where you draw that from is beyond me?
I know where I'd sooner have lived along with those I care about during the pandemic... and it's not just because of the better weather down there.
Will be interesting to see how that looks in 6 months tbh
It really will. Very high vaccination rates. So high in fact that a lot of the deaths are vaccinated people, but with comorbidities.
Queensland has just this hour decided to let international travellers back in without quarantine too. Will be good to see my folks at some point.