Some of the features of Covid 19 and people's reactions to it, or why it's such a successful virus:
Many people don't even know they have it. Another group of people have none of the classic symptoms but very mild symptoms that could easily be confused with other mild ills such as allergies or mild colds.
Many people refuse to change their habits or isolate even when they test positive, it's on the coronanomics thread.
Many people with symptoms don't test and carry on as usual.
It's highly infectious, contact with surfaces, airborn, even fine aerosols from breathing can transmit in indoor spaces.
People are infectious before they show symptoms.
It's spread worldwide, even if one country has a radical attempt at elimination and succeeds it will then become isolated from the rest of the world because of the need for long quarantaine periods to avoid recontamination.
The vast majority of countries have opted for management strategies rather than elimination. They're all in search of the grahl, measures that maintain R below 1 without provoking economic depression and social chaos. And to make measures work they have to keep the public on side. Measures have to be seen as constructive rather than punitive.
Suggesting measures is fine, make sure they stand up to examination because if one makes a suggestion on a public forum one is inviting the public to comment on it.
I might be a non-payer but you'll find logic, realism and pragamtism in what I post. With facts to back it up from all over Europe.
How about splitting the forums (fora?) into two parts?
Paying (full) members and non-paying (free) members.
If you’re a paying member that gets you full view and comment access.
If you’re a non-paying member you can only view and comment on posts from other non-payers.
It sometimes feels that threads are dominated by non-payers – to the detriment of paying members.
Not even sure where to start with this. A very bad suggestion! (From an on-and-off subscription payer and long term forum lurker)
There's too much noise about this carry on. Couple of simple points that everyone in the country should be very angry about. The tories are making an absolute ct of this... again. And they are also refusing to pay for the necessary action going forward, ie supporting people and business.
We really should be kicking down the doors of downing street right now.
The warning signs have been there for over a month now.
Dither and delay, eh...
There are countries at level 1 in that old chart… but we’re still pretending it’s not possible… because we can’t be arsed to spend a month or two making it happen… so we’ll stay near top of what chart all winter, destroying what’s left of many sectors and counting the job losses and ignoring the cost of the “do as little as possible” approach in the long term.
I would somewhat agree with this.
None – eradication is not an aim for SARS-COV2 management. It isn’t going to happen
I'd also agree with that
No country that’s had the level of cases European countries currently have spread over their entire territory has got back to single figures.
And kinda agree with that.
This is something we have reflected on quite a lot here in Australia - seeing the complete balls-up the UK is continuing to make of crisis management. The sad fact is: the window for action needed to be level 2 today (and be pursuing level one) was in March. No way you can get there now because of the lead-in of incompetence and mismanagement.
The things that Australia and NZ are doing now to get to level 2 and 1 are only possible because our number of cases are so low - you're never going to get there from where you are now. They are only possible because of the steps that were taken back in March and April - and more recently in Victoria (which is another story).
A good example is track and trace. Yes we have an app over here - but the REAL tracking and tracing is done by a team of humans - they interview every positive case, find out who their contacts were, and go and chase them down for testing. Our premier (state governor) stands in front of the press every morning and tells you where the 3 new cases in NSW over the last 24 hours have been found, tells you where those people went whilst infectious, what bus they rode on, which Cafe they went to etc etc. Appeals for anyone who may have come into contact with them to come forward. We had a positive case in my neighboring suburb - a young lad working in a local (big) supermarket whilst infected. They set up a pop-up testing clinic in that suburb - no appointment required, don't need to have symptoms..... just come and get tested (thousands did) - results back within 24 hours, so people aren't dissuaded by having to self isolate for too long after getting a test.
And even that's not enough to get down to zero. In New South Wales, we've just had 14 days of zero "community transmission" - but that run's been broken by 5 new cases today. Even our goal is not eradication - our goal is to keep the numbers down by track/trace/test/isolate, so that life can continue with as few restrictions as possible.
I think all that you can hope for in the UK is that you hang on by your fingernails (both in terms of economy and health outcomes) until a vaccine is available.
I think all that you can hope for in the UK is that you hang on by your fingernails (both in terms of economy and health outcomes) until a vaccine is available.
Yep, what was it, 30% of contacts not traced last week? Its not working and we must be spending millions on a system that doesnt work.
The problem isn’t hysteresis and lags, the problem is it’s highly virulent due to presymptomatic infection and anything short of a severe lockdown just isn’t enough to keep it in check.
It started increasing in July when pubs were reopened, despite what the SAGE idiots were saying at the time. Add in schools and an increase in workplace attendance, it was only ever going to go one way.
anything short of a severe lockdown just isn’t enough to keep it in check.
See my post - we are not in severe lockdown, and we are keeping it in check. This is the case in lots of other countries. A severe lockdown is required BECAUSE it hasn't been kept in check.
Remember the idiots in SAGE told us that R was less than 1, all through July and August when we could see the number of cases increasing steadily. About two doublings from 400 to 1600 per day before they even noticed. ****ing muppets.
Meanwhile, back in gravytrain land, we're paying for a thousand Deloitte consultants for our world beating test and trace fiasco system.
There does seem to be a deliberate policy of keeping quiet about coronavirus in schools. I can't think of another area of daily life where so many people mix so freely without social distancing.
It started increasing in July when pubs were reopened, despite what the SAGE idiots were saying at the time. Add in schools and an increase in workplace attendance, it was only ever going to go one way.
was it not just last month they were saying ---- back to work if you can - Keep Pret in business !
- We just had an email out saying no attendance to office or workshop without expressed permission from management and QHSE UNTIL january 18th 2021
And our "world beating" test and trace thingy has apparently only sent *one* alert about an infection at a pub:
Money well spent.
It started increasing in July when pubs were reopened, despite what the SAGE idiots were saying at the time.
It’s very hard to see from hospital admissions much of an inflection, but the eye of faith hints at a slight (and I mean very slight) deviation from log-linearity at early to mid August. It’s a pretty subtle effect though.
The obvious inflection at the end of August and early September is highly correlated with schools.
The failings of the systems and processes by all responsible are clearly not helping, but no matter how clear the rules are, how well they are understood by everybody, there is a significant proportion of the populace who will never follow them. They just don’t care.
I commute through Newcastle every day. In all of the common areas there are groups congregating (mostly 16-25 year olds); kids are playing in the streets/play parks as normal with their mates; and in retail there are people mixing indoors (all ages) from more than one household (unless same-sex relationships are now the majority).
It’s not a surprise to see Newcastle struggling with rising infection. I’m surprised it’s not higher.
No rule changes will change this behaviour for these people, apart from a total lockdown. I’m not qualified to know if that’s a good idea, but it’s the only option, based on what I see every day.
And [s]our[/s] English & Welsh “world beating” test and trace thingy has apparently only sent *one* alert about an infection at a pub:
Speak for your own country.
There does seem to be a deliberate policy of keeping quiet about coronavirus in schools. I can’t think of another area of daily life where so many people mix so freely without social distancing.
I dont think any other workplace would be allowed to reopen without PPE or distancing.
Remember the idiots in SAGE told us that R was less than 1
I don’t subscribe to the cult of R. I consider it inestimable other than >< 1 due to its confounding with other factors such as period of infectiousness. I do however believe that exponential processes are best viewed on logarithmic scales.
I think we are about to find that schools are a significant contributor to transmission, which is the null hypothesis from influenza. The beauty of looking at england is the sample size and reduced fluctuations compared to Scotland, Wales and NI.
The ONS and React studies both show no rise in community infection during August, I put up my analysis a a week ago of React. There’s at least a week lag between policy changes and rising cases/admissions just due to incubation.
I think we are about to find that schools are a significant contributor to transmission, which is the null hypothesis from influenza.
If by that you mean this was blindingly obvious from the start, I agree.
Problem is we are so far down the road of schools business as usual changing tack will be very hard both for Boris and chums and schools.
matt_outandabout
Full MemberAnd our English & Welsh “world beating” test and trace thingy has apparently only sent *one* alert about an infection at a pub:
Speak for your own country.
My sincerest apologies. Have you really not gotten around to leaving yet?
If by that you mean this was blindingly obvious from the start, I agree.
Indeed. SARS-COV2 transmission = influenza transmission is the null hypothesis. Not seen anything to reject it on the macro scale so far. A lot of heat and noise about whether children are infectious, suffer morbidity and mortality. But I think it will come down to what we first suspected - which looks like influenza - normal transmission with lower morbidity than influenza.
there is a significant proportion of the populace who will never follow them
And no one seems to have a clue how to tackle that behaviour, so we just seem to shrug and ignore it.
It's now a week since my lads college had it's first student with a positive test. Picked up on a random ONS test 12 days ago, was in school for three days showing no symptoms before their results came back. Close contacts at school all told to isolate.
Thus far, no reports of any more positive tests linked to it.* It's a strange one, transmission in school. Or a lottery.
*Assuming this poor 17 year old isn't single handedly responsible for Nottinghams wider problem this week!
All the data I’ve seen points to 18-30 transmission rather than school age?
I must have missed this a week or so ago - really fascinating study.
If the findings are robust, it could help explain so much of why certain countries, and subgroups of their population, have been hit so hard. Obviously, it's just one potential risk factor for severe illness among many - age, weight etc.
So basically, prevalence of this particular gene is higher in parts of Western Europe and South Asia, and lower in Asia generally.
So, it's possible that it could be one factor that makes people of South Asian descent in the UK much more likely to get really ill and die from Covid. And more generally, one of the reasons why Asia seems to be doing better than India.
One interesting nugget is that one of the areas with the highest prevalance of the gene in Europe is northern Italy.
Having certain genes of neanderthal origin apparently makes you more prone to T2 diabetes, and inflammatory conditions such as lupus, which hints that you may be more likely to mount the wrong kind of immune response to Covid.
All the data I’ve seen points to 18-30 transmission rather than school age?
Data wont exist if kids dont get ill
Interesting link on outbreaks in schools, not exactly mainstream national media though, so it does feel like there's a policy of non reporting https://www.watfordobserver.co.uk/news/18769542.coronavirus-outbreaks-england-spreading-mostly-schools/
Interesting graphs that I can't seem to show as images, sorry.
From sky news.....
A widely-circulated open letter calling on governments to pursue herd immunity is counting homeopaths, therapists and fake names among its "medical" signatories, leading to accusations that it falsely represents scientific support for the controversial position.
The Great Barrington Declaration, a letter organised by prominent advocates of herd immunity, claims to have been signed by more than 15,000 scientists and medical practitioners, as well as more than 150,000 members of the general public.
Yet Sky News found dozens of fake names on the list of medical signatories, which anyone can add to if they tick a box and enter a name. These included Dr. I.P. Freely, Dr. Person Fakename and Dr. Johnny Bananas, who listed himself as a "Dr of Hard Sums".
I don’t subscribe to the cult of R. I consider it inestimable other than >< 1 due to its confounding with other factors such as period of infectiousness.
><1 was precisely the point. They said <1, the data said >1. SAGE also published daily growth rates which are more directly interpretable and which were just as obviously wrong.
Hospital and death rates lagged because the growth was initially in young adults, who don't (much) go to hospital or die.
SAGE member Jeremy Farrar is now going around saying "told you so". The facts show very clearly that this is not the case.
MPs to get a £3300 pay rise next year. Absolute ****ing disgrace
Interesting link on outbreaks in schools, not exactly mainstream national media though, so it does feel like there’s a policy of non reporting.
This is kind of stuff they need to be publicising to explain where they are with policy. Mind you, less than 300 cases out of 782, not clear if it's kids being infected or teachers, so still more detailed investigation needed. By real people on the ground, not by apps or Servo call centres.
“Dr of Hard Sums”
Damn! found out... I wouldn't take these signatory things too seriously. I would, however, consider the merits (or otherwise) of the arguments. I simply do not subscribe to the immunity view (that Gupta has backtracked from), and nor do I believe we can "protect the vulnerable". We do that each year with influenza. Some years it works well, others less well. And as someone with morbidity, I still think we know so little about the disease of SARS-COV2 infection (beyond pneumonia). It is far too early for sweeping generalisations.
Feynman summed it up: “if you thought that science was certain – well that’s just an error on your part”.
You might like to read this week's NEJM Editorial. It pulls no punches. Utterly damning.
the growth was initially in young adults, who don’t (much) go to hospital or die.
It didn't really show in REACT and the ONS data - but age breakdown is only from mid August. But it is also fair to say that the testing was so confounded as to be unreliable (and still is). If pressed, I would say that we had R on the run at <1 until late July, Then 1 or thereabouts for low daily incidence with gentle increase over August noted in the younger generation. That is the hysteresis - then a big acceleration with schools opening. But I model the data, I don't estimate R.
Ignore my earlier post - college update just come through to say they've had four new cases this week, but none are connected to each other or last week's case, so no evidence of in college transmission.
Starting to feel like a game of creeping death.....
that indie sage 😬😬😬😳. Hospitals in the north to hit same admission rate as London on march lockdown day in a week!!
REACT-5 data released today from Imperial. Last Friday it was "Some evidence that the epidemic growth was slowing down". I believe the scientific term is retraction...
My analysis of the full data below. @thecaptain see (with the eye of faith) if you can spot the rise in August - the model is an exponential growth/decline cubic function through all the observations.
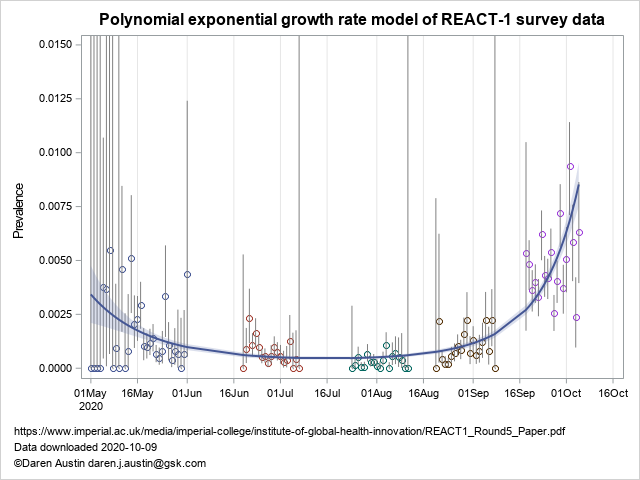
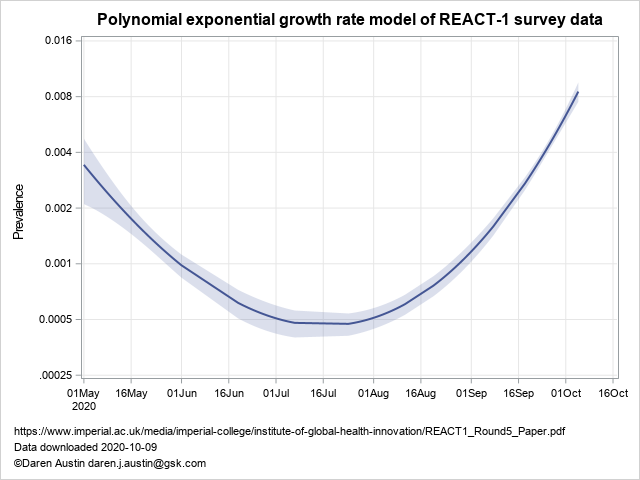
On a log-plot, the nadir is in fact the third week in July, but some uncertainty of course. Plotted on a log-2 scale so you can read off the doubling time, which is about 4 days.
Hospitals in the north to hit same admission rate as London on march lockdown day in a week!!
That was what I was warning about. Focus on the national numbers, especially the tests from a stalled testing system, and you miss where we really are. Any chance of some regional admissions graphs TiRed?
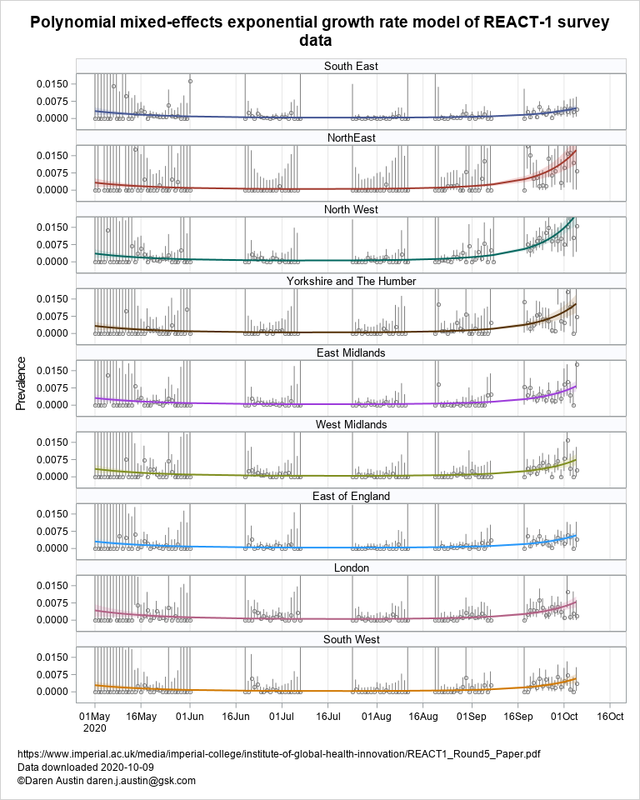
Regional REACT data on prevalence - spot the high prevalence regions. I haven't processed the admissions data fully yet, but have been meaning too. The source data is a bit dirtier.
REACT regional data
We can debate the precise date of the bottom @TiRed and I agree that case numbers aren't the whole truth but remember SAGE was saying R<1 right through to the end of August. That was unforgivably poor advice.
I also wouldn't choose to use any particular polynomial though and would instead do a more epidemiologically-based model fit with time-varying parameters. I'm puzzled why the REACT team haven't done this and suspect it may be because they don't know how to. Which is disappointing as it's a very well-established approach. The piecewise-constant R approach they have implemented is really very limited and has generated some very silly results (like when they said R was 1.7, then 1.1 - and regardless of your feeling about R, the resulting doubling times were just as silly).
Just seen this tweet on the bikeradar CV19 thread, no idea how reliable it is...
https://twitter.com/Smyth_Chris/status/1314593156852256768
Bit of an 😮 moment, if true.
Etiquette question: is it rude to glare at maskless people on the train?
Yup that's about right. It is a slightly unfair comparison in some respects however, in that the exponential rate of increase was much greater then, and our treatment options and general preparedness is probably rather better.
SAGE was saying R<1 right through to the end of August
I thought they were reporting a range, with the upper bound being above 1, throughout August. That may have been oversimplified by media and politicans alike, but “we” should have been acting based on the range, not the mid value. Many of us have been.
It is a slightly unfair comparison in some respects
True, but if, currently, the virus is more prevalent among groups less likely to present at hospital, than in Feb/March, it would be foolish to ignore under react in response to the rise in admissions now.
Etiquette question: is it rude to glare at maskless people on the train?
Yes it is. Surprised anyone needs telling that. Do you also go round checking that people parking in disabled spaces have a proper disability?
I also wouldn’t choose to use any particular polynomial though and would instead do a more epidemiologically-based model fit with time-varying parameters.
They've reported pairwise interpolations from one to the next survey, which gives the same as an exponential polynomial. When the rate is relatively low the polynomial and exponential models are the same - which is why I use them. PHE I believe use a spline fitting method to do the same. I believe the group are interested in epidemiological models too, but for robust reporting they have relied on single survey and two-survey log-linear regressions using a binomial distribution. Then they adjust for the sample survey bias to get a population estimate. the above is unadjusted.
As for the epidemiological models I think we are at the point where the time-varying part is now where the degrees of freedom fall. So many options can give the same goodness of fit, I consider them to not be robust. I worked up a paper on immunity using SEIR models and uncertainty - the issue is really what one wants to assume about intervention. The very succesful COVID-predictions webpage page has closed for further prediction for this reason - the author was spending too much time tinkering to keep up with interventions.
Yes it is. Surprised anyone needs telling that. Do you also go round checking that people parking in disabled spaces have a proper disability?
No but if mis-parking risked transmitting a fatal disease I well might.
