For me the difference between placebo and relenza is daytime tv. On placebo I’m in bed feeling really terrible. On relenza I’m downstairs feeling like watching tv. IV relenza is also approved for severe disease though.
Trouble is that even if avigan etc show a positive effect on disease progression the scale up of production will just be insufficient against demand.
They are talking about 100000 doses available in July rising to 300000 in Sept.
At this rate the US would take them all and not touch the sides
Would these drugs - if proven- be globally manufactured?
You would hope they would be licensed yes. I will say I don't know anything about the structure or manufacturing process of that drug but as it appears to be a small molecule they tend to be easier to produce as they are a synthesis product so there are less variables to cause issues with production.
trouble is who tests them as methods have to be transferred and labs have to be approved.
thankfully if the fuji one works it is a small molecule so scale up is easier than biologics.
I just can't see a way that these would not be rationed once released at least for some time. Will take time to get enough doses to be able to have in the same way as tamiflu.
To summarize what's happened in my lab this week, we're still limited to 35 in house tests per week because there's still not enough availability. We started sending all the remaining swabs to one lab (rather than splitting them between two) because a new platform had been installed, but they ran out of reagents within a day so all the swabs ended up going to the other lab. Theres was also a lot of discrepancy between kits i.e. some tests were positive in one, negative in another.
We are at the limit of how many swabs we can process purely down to the time taken to receive, process and send them on. We don't have enough staff to handle it. In house testing is quicker, but we don't have the allowance to meet our demand.
We may well be at 100,000 tests nationally, but it's far from plain sailing and the "mega labs" are likely to be taking some of the kits that we could do with in NHS labs.
There's also concern about the quality of their work. The labs are staffed by volunteers whereas NHS labs are staffed by registered biomedical scientists and are UKAS accredited. Also, how do those test results link back up to NHS systems. Our labs are barely linked together as it is without introducing the private sector.
They are talking about 100000 doses available in July rising to 300000 in Sept.
At this rate the US would take them all and not touch the sides
India to the rescue! ? china? They'd have capa city to really ramp up?
chasing a magic bullet, anyway, 20 years in cancer research & I'm over that one!I
realistically What's the chance of that working, I'm not clued up on what these drugs are targeting, is it blocking the cytokine storm seen in worst patients or inhibiting virus at earlier stage?
Is a 1 drug fits all solution even likely? I suppose It's best near term.goal, but realistically it's gonna be a combination of therapies, tailored to whatever the patients immune make up(not easy to.mass test for?) & comorbidities dictate.
Theres was also a lot of discrepancy between kits i.e. some tests were positive in one, negative in another.
@richardkennerley what kits are you using?
It's a bit weird, I live in MK & volunteered for national testing centre they've set up here (and where they've taken out institutes machines to), but not heard anything back, colleague with less (virtually no) qpcr experience but lives in London has been asked to work there &they'll put him up in a hotel
The fuji one blocks or inhibits the rna dependent rna polymerase (although according to the wiki link below it might have multiple modes of action)
https://en.m.wikipedia.org/wiki/Favipiravir
https://www.europeanpharmaceuticalreview.com/news/116981/production-of-avigan-tablet-favipiravir-accelerated-for-use-against-covid-19/
That is a pretty big loading dose too 1800mg (horse pills)
I'm not sure what the regional lab is using.
We've just got Cepheid up and running, it's excellent. Currently got 4 slots but hopefully will have 8 soon. Each slot knocks out a result in 50 mins. If we had full availability we'd be able to do 150 a day. If anyone saw BBC news t'other day when they were talking about testing in Shetland, it's the same kit.
We've also got a Qiastat on which we can run a full respiratory screen plus covid in 70 mins. Very limited kits on that, reserved for haematology patients primarily.
One for me to read up on over the weekend. There's lots of talk of vaccine trials. Do they proceed in the same way as drugs trials? It seems the early phases would be similar, ensuring they don't do harm. But how about later stages. How do you ensure they are effective. I'm guessing the small pox approach isn't considered ethical so is it a case of monitoring antibodies? How about timescales of effectiveness and harm Can you only say it is safe/effective in the time frame in which you've studied it or are there accelerated/indicators for longer term (antibody concentration decay or something?).
If you find any good links on the current vaccine trials post them up.
I saw an article the other day where they said that the dropping infection rate would inhibit the trial, so am assuming they are running the covid ones in a similar way to the ebola emergency ones, basically give it to people and assess safety and see if they get sick from the virus.
I could be totally wrong in that though, as haven't had time to do any reading.
I could be totally wrong in that though, as haven’t had time to do any reading.
From the timescales being talked about, I don't think they have much choice other than to skip normal safety checks
Vaccines are approved based on proven efficacy. Not on ability to raise an antibody response. The current trials are proof of concept to show that antigen presentation generates an immune response and some antibodies. Efficacy trials are next. They require large populations to assess safety, and a control group to show protection rate. The challenge will be what happens when the virus has declined. Can a protection efficacy trial still be conducted?
Passive vaccination with an antibody also requires efficacy trials. There is a route to approval using the animal rule, where an exposure that is protective in animal challenge studies is assumed for humans. The anthrax antibody raxibacumab was approved via this route.
It is entirely possible that we fail to produce vaccines and drugs because control measures (needed due to their absence) have worked too well. Interesting dilemma, no?
Thanks tired. I think I need to figure out a way to get over to wavre or rix to do some learning.
Yeah that could be an unfortunate dilemma as it would be totally unethical to do viral challenge studies without an effective antiviral drug incase the infection went too far
This whole testing business is depressing isnt it. Gov massively ramps up testing in response to a Minister saying something stupid which just proves that had they tried to ramp up testing capacity in Jan or Feb we could have saved what? 5 000 lives, 10 000 lives, 20 000? Could we all be looking at going back to work and school in the next week or so? Am I being overly harsh on the gov? Surely they are going to start being held to account soon, when do opposition parties wake up, when do journalists start asking real questions?
You’re not being harsh. Failure to devolve testing has been the biggest failure in my opinion. I think the government have got most things about right. But not testing. PHE will not come out of this well. It’s limited available options like no other decision.
What goes around comes around.
I think the government have got most things about right.
The thing is though, they looked at Italy, said we were two weeks behind but then didnt act, they accepted the oncoming shit storm rather than act differently to italy and spain and didnt try to "flatten the curve" then. They set a target of 20 000 deaths as a good result and shoved their collective fingers up their arses and now it looks like what 40 000 will be a good result for the first wave? Unless they have learnt lessons, which I'm not sure they have a second wave could be as bad or worse.
To be honest, any prediction of the cumulative effects of an exponential process within 50-200% isn’t bad. Most people don’t understand just how nonlinear epidemics really are.
We will be about the same as Italy. Sub 40000 deaths in hospitals and nursing homes would be a good outcome, and equal to a bad influenza year. And that’s with lockdown. Think of what it would have been without. That is the perspective that’s needed. Total 2020 excess deaths of 50-75,000 is likely. Assuming a modest or absent second peak.
A-A - you've just asked for opinions, got one from probably the most qualified and experienced person on the thread, and then started some whataboutery because it doesn't seem to fit with the answer you were hoping for?
My own personal view on the government's handling is probably harsher than TiReds, but I'm prepared to accept his opinion.
It is entirely possible that we fail to produce vaccines and drugs because control measures (needed due to their absence) have worked too well. Interesting dilemma, no?
Adrian Hill of the Jenner Institute covered that paradox a couple of weeks back on ITV's (sometimes) excellent CV podcast:
(It's the "GPs could 'quite possibly' have Covid-19 vaccine by Christmas" episode.)
I think the government have got most things about right. But not testing. PHE will not come out of this well. It’s limited available options like no other decision.
They wanted to centralize testing so testing availability was stifled and that lead to a bottleneck in testing. Is that a fair criticism though? Germany's testing was totally distributed which meant they did a lot of it. But the trade off is a lot of their testing was performed by random clinics on random people where there was no suspicion of CV. Just like us Germany suffered from a shortage of reagents (and swabs!) so wasted tests were a big deal for them. Plus they had no central control of testing to the point they didn't even know how many tests they were doing. On the face of it PHE got it wrong but I wonder if a rational assessment in the future will conclude they behaved reasonably? Letting the market do your testing has advantages and drawbacks, just as centralized state testing has advantages and drawbacks.
...and if it was obvious from the start that the free market is inherently better at testing then why wouldn't you think the free market is inherently better at treatment?
Having said all that PHE will come out this with a ton of blame just like everyone else, I'm sure.
A-A – you’ve just asked for opinions, got one from probably the most qualified and experienced person on the thread, and then started some whataboutery because it doesn’t seem to fit with the answer you were hoping for?
Its called a discussion all I've done is ask questions, if you dont like that feel free to ignore me.
To be honest, any prediction of the cumulative effects of an exponential process within 50-200% isn’t bad
I understand that any exponential process is going to be hard to predict. My question is could with proper planning we have avoided the exponential process like Germany has to and extent. I want people to help me understand why Germany is different from us, why Portugal is so different to Spain and why Italy didnt act like a rocket up our arse?
you’ve just asked for opinions, got one from probably the most qualified and experienced person on the thread, and then started some whataboutery
True, but TiRed should have spotted the bait IMHO, it was pretty obvious.
We will be about the same as Italy. Sub 40000 deaths in hospitals and nursing homes would be a good outcome, and equal to a bad influenza year. And that’s with lockdown. Think of what it would have been without. That is the perspective that’s needed. Total 2020 excess deaths of 50-75,000 is likely. Assuming a modest or absent second peak.
Think we cross posted, the thing that stands out for me is think about what happens without lock down, but lock down was the only option, locking down earlier, would that have helped, testing and tracing more and for longer would that have helped. It feels to me that the gov planned for deaths on massive scale and thats what happened/is happening.
True, but TiRed should have spotted the bait IMHO, it was pretty obvious.
Feel free to ignore me.
why Italy didnt act like a rocket up our arse?
The rocket up our arse was the ICL report by Professor Neil Ferguson et al. That 500k number changed everything. I assume that was strongly informed by numbers from Italy.
So Italy *did* act like a rocket up our arse.
So Italy *did* act like a rocket up our arse.
Feel free to ignore me.
I want people to help me understand why Germany is different from us
The various reasons have been endlessly reported and can be googled:
https://www.nytimes.com/2020/04/04/world/europe/germany-coronavirus-death-rate.html
Letting the market do your testing has advantages and drawbacks
Capacity being the advantage. Hancock should be thankful that industry saved his bacon.
The other societal and industry failing is why after SARS-COV-1, do we not have a Coronavirus treatment. Not a vaccine, those seem hard (forget the media noise). Clearly there would’ve been limited market for an unspecified future pandemic. There are means to approval even when a pathogen is not rampant. We have antivirals for influenza because epidemics are annual. We don’t have antivirals for coronaviridae. Or flavivirida (Zika). Or arboviridae or most others. I looked at some other possible therapies yesterday.
Oh and I don’t take debate personally btw. Always happy to discuss from a factual point of view. AA is always one of the good guys 🙂
The various reasons have been endlessly reported and can be googled
Feel free to ignore me.
The media story is currently about whether 100,000 tests took place on one arbitrary day (chosen by the government), but I for one was just happy that testing capacity has been ramped up, almost forgetting that this should have happened ages ago, when the government abandoned testing beyond patients in bed (and royals and politicians) as a strategy when WHO were saying “test, test, test”… and then I was reminded that we are being played…
[img] 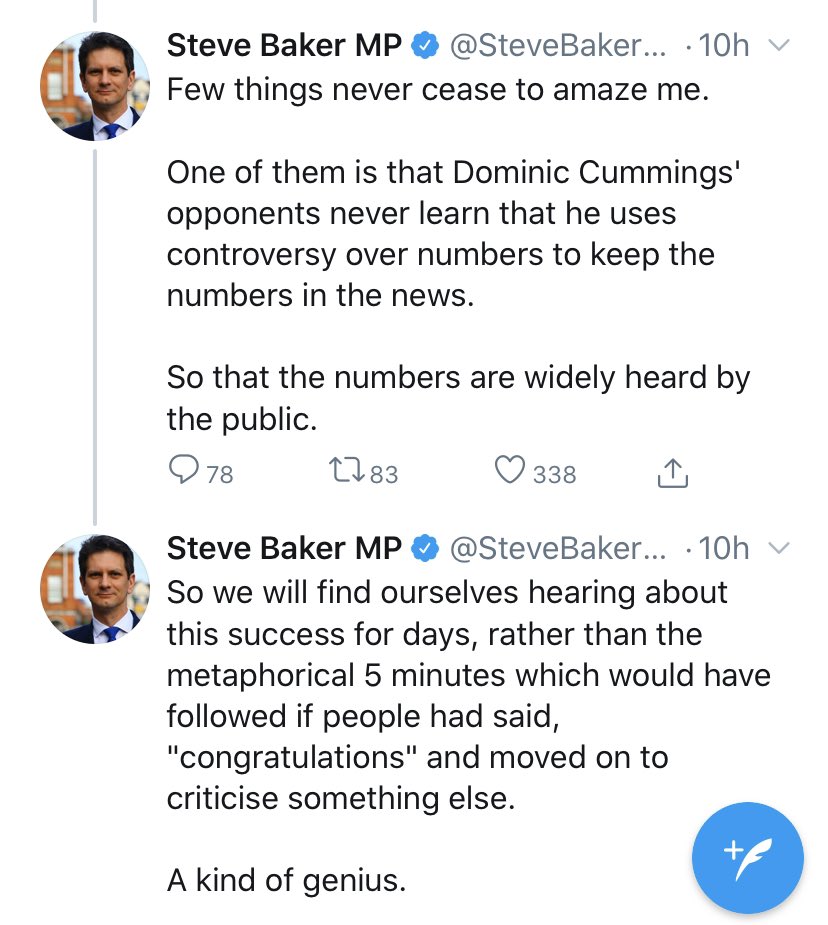 [/img]
[/img]
Off out for a ride. Tired thanks for the input, I'll get back to you with a few questions later maybe via pm if thats ok, it stops people getting upity.
Enjoy the ride. I’m still suffering a sore chest. So a sunny walk with the dog will suffice. And don’t forget that AA has the important job of trying to make sense of this to the next generation. There are enough biology lessons from this pandemic to fill a term!
The other societal and industry failing is why after SARS-COV-1, do we not have a Coronavirus treatment. Not a vaccine, those seem hard (forget the media noise). Clearly there would’ve been limited market for an unspecified future pandemic. There are means to approval even when a pathogen is not rampant.
How do you conduct efficacy trials against a coronavirus that either doesn't yet exist, or has been eradicated from the population? I suppose you could trial it against common cold coronaviruses, but then these are generally trivial in terms of respiratory problems, plus most people have some degree of immunity.
Do you mean a list of candidate treatments tested against SARS or MERS in the lab environment, ready to roll out into humans should a novel coronavirus emerge?
Exactly. Antivirals attack various points in the replication chain. So they can be tested one w out have the poster child in the lab. The SARS-COV-2 virus is 59% identical to the previous virus. Then you test efficacy in animals and safety in humans. That is the animal rule. BARDA have been all over this for years.
@seadog101 My approach would be that it's no one else's business what you do (as long as you're not coughing on anyone or failing to observe distancing). Crack on the busy bodies can get to ****!
Stay safe and well!
Ask publicly AA please, most people are finding the replies interesting, I would have thought. Apologies for the occasions when I’ve been one of those who got uppity with other posters, keep talking.
I got banned over my last comments on Outofbreaths contributions. So I reckon A-A has the right approach going private.
Talking is fine but we need to be able to call out people talking stuff that is plain wrong without being handed a ban.
So Germany is planning widespread random testing for antibodies in the future but it has not had random testing up to now. This:
Germany’s testing was totally distributed which meant they did a lot of it. But the trade off is a lot of their testing was performed by random clinics on random people where there was no suspicion of CV.
is simply not true.
There should be nothing wrong with calling out errors. Just have to play the ball not the man.
I think a number of us have slipped over that line recently
Lockdown seems to be over anyway.
After De Pfeffel's cretinous utterances the other day there is a strong whiff of '**** it, we've had enough of this'.
I could have got it wrong of course. I mean, the LGBT mountain bike riding and rambling scene around where I am doing my no car, no gnar and not far might have been much bigger than I realised all along. Or there could be lots more adult siblings living together than I thought.
Or, more likely, as one of our regular scottish(?) posters put it:
"Lockdown my arse".
Exhibit 1: Three 40 odd year old women jogging together down the road. No distancing.
Exhibit 2: Two 25 odd year old blokes, one with helmet, one not riding two abreast along the road chatting. No distancing.
Exhibit 3: The two old dears and their dogs I regularly say hi to and know are not from the same house. No distancing.
Exhibit 4: As exhibit 2 just with different cast members. No distancing.
Exhibit 5: As exhibits 2 & 4 but this time both wearing helmets. No distancing.
Depressing that cyclists (and not roadies this time) were 60%.
Now we can do the whole "you mustn't jump to conclusions" thing, but before/if you do please ask yourself one question:
Would I put £100 of my own cash on a bet that all five of those adult same sex groups comprised members from the same household in each instance?
Edit: Should also have mentioned that these groups were all out and about very early. Almost like they had something to hide. And that road traffic was up at least threefold on last week.
A lot of people do seem to be slipping, I guess we will see how much by looking at infection rates.
I think a number of us have slipped over that line recently
I have, for sure. I’d like to apologise again. I don’t know why you got a ban, but I can think of a few occasions where I was lucky not to receive one.
is simply not true.
I took it to mean ‘not targeted efficiently enough’, rather than random testing. Which may we’ll be true, but not really such a problem if you have enough capacity for testing. Our testing has been ‘targeted’, and that held up as a ‘good’ thing… but the reality is that our ‘testing strategy’ means that we are now pretty much in the dark about the UK situation outside hospital beds, and will he relying on models using data from other countries, where the spread in the population is likely to be quite different to here.
A lot of people do seem to be slipping, I guess we will see how much by looking at infection rates.
And we are back to playing catch up with community testing, tracking and testing. The one thing that is currently winding me up, is Hancock now repeated stressing how important this is… WE KNOW, YOUR PREDECESSOR (and WHO) TOLD YOU MONTHS AGO WHEN YOU STOPPED DOING SO.
I think the government have got most things about right.
Yeah you said that before but it’s hard to take seriously - like on lockdown timing, dropping testing, dropping any plans to get tracing going in a big way, not preparing PPE, not giving attention to care homes. I mean apart from that yeah they did great.
like on lockdown timing, dropping testing, dropping any plans to get tracing going in a big way, not preparing PPE, not giving attention to care homes
I think they are currently getting much ‘right’, but got all those things wrong when it mattered. We have thousands of extra early deaths that could have been avoided if certain ‘data scientists’ had less sway early on… when mitigation measures, which were always going to be required from the moment the first cases appeared in Europe, where needed as early as possible to reduced the impact on lives and the economy.
How do we think the government will relax the lockdown while keeping R<1?
Is it even possible?