Forum menu
Some interesting reading related to @kelvin's post above.
The study, published in the New England Journal of Medicine,1 found that vaccine efficacy between the first and second doses was 52% (95% credible interval 29.5% to 68.4%), with 39 cases of covid-19 in the vaccine group and 82 cases in the placebo group.
- https://www.bmj.com/content/371/bmj.m4826
Note the wide interval.
The second estimate comes from the UK's Vaccine Committee, the JCVI, who decided to calculate the efficacy of the vaccine differently. Instead of using all the data on the number of infections, including from days when the first dose hadn't yet started to work, they only looked at days 15-21. Using this method, the efficacy of the vaccine jumps up to 89%, because it's not being diluted by the relatively high number of infections before the vaccine begins to have an effect. Taking things even further and only looking at the first seven days after the second dose (days 21-28) – because the second dose might not have kicked in yet by then – it's 92%.
However, these calculations are controversial.
- https://www.bbc.com/future/article/20210114-covid-19-how-effective-is-a-single-vaccine-dose
Fun with stats!
Reassuring though, thanks impatientbull.
However, these calculations are controversial.
Flawed would be my judgement. There were TWO, yes two infections in the active group between days 15-21. Two more from 12-21. So extrapolation was based on four events. 39/82 is a worst case scenario because there is no separation early on.
This is my day job, and I'm concerned. I would not have used such an analysis, personally, for such an extrapolation. The data is just not robust. The Moderna data is much stronger.
There is also no data from Israel so very early days yet.
EDIT: Below is the clinical data. Imagine moving those four events around a little (the already look clustered in pairs) and then projecting forwards...
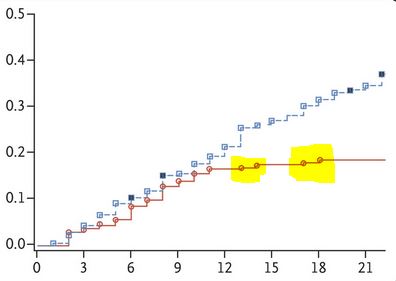
You don't need modelling to see that guessing later than 21 days is challenging
ok, so this page is back on track, however the increasing infighting on p604 clearly shows the impact of this T3/T4/LockDown across the board. Glad that STW is not very representative of the population at large.
I’m less reassured now.
When stats look like wishful thinking interpolation to support hunches.
Truth is, the numbers of infections involved in the trials are not large but they are statistically significant.
I personally have an issue with some of the end points used in the mrna vaccines, but I think the calculations on delaying the second dose are more on providing lots of people some protection against very high protection in a smaller number of people.
Not convinced that is a great plan considering the death rates reported in care homes etc
I’m unsure whether it’s a good plan or a bad one… only time will tell… but I’d rather it was supported by evidence rather than a hunch… I’m highly sceptical about the political motivations behind it still.
What I think should happen now (but won’t) once the dust has settled is that the PM should make a thank you speech to the youth of the nation that got it right acknowledging that they have had the least to lose but had the biggest impact on their lives and finances. 16-24 years olds should get a £XK thank you to rebuild some of the damage done to their education and embryo careers. Only caveat – if you were in receipt of a penalty fine for breaching covid restrictions you miss out. There should then be an equivalent X% rise in income tax on monies earned on pensions for the next 10 years on top of whatever income tax we are all paying by then.
The message should be loud and clear that it was a team effort to get through this but it is a team effort to pay for and make good too and that the oldies need to appreciate that whilst they might have had the most to fear from the virus those that did not die have not had their lives turned upside down quite so much as the young that did the right thing to protect them. That debt now needs repaying.
On a general population level the maths if the numbers are right should work.
But with the groups that are at the highest risk of death i wouldn't be happy.
50% of say 4000000 is 2000000 protected, 90% of 2000000 is 1800000. But that's assuming efficacy numbers and is a horribly general way of putting it.
Either way I'm not sure.
Truth is, the numbers of infections involved in the trials are not large but they are statistically significant.
The effect is large and very well-characterized BEYOND 21 days. But up to 21 days, it's an educated guess. Believe nothing else. I told Matt Keeling at Warwick (on JCVI) this a few weeks ago, and he repeated it on More or Less on Radio 4. I was working on a more robust inference method for extrapolation, but when there is little data, the method won't help!
@tired when will we have some data and info around whether the vaccines provide sterilising immunity?
There is limited evidence on secondary infections in the Oxford trial (from memory they halved), but otherwise it will be many months for population-level data. To be blunt, we are vaccinating those who would die.
One month: Expect to see the proportion of deaths in >85+ fall first, then 75+, then 65+.
Three months: Expect to see the age distribution of hospital admission change to younger age groups, because when the 75+ are protected, they won't go to hospital, then the 65+...
Six months: Expect to see the age distribution of cases change to lower age groups. Only then can you really start to infer transmission reductions.
For the record, I don't expect a high degree of sterile protection from the Oxford vaccine. Some, maybe 50%, and this may halve R from 4 (new strain) to 2, maybe 1 and a bit with herd immunity. Reinfection is noted from the recent study, so I predict that infections, possibly some symptomatic, will again be the case for the vaccinated. But, and it is a big but, they will not need hospital.
So im just jumping back into this thread from a while back but the last two pages don't read too good to me?
Sorry I should have been clear that I meant up to 21 days post initial vaccination in my post
1820 today 🙁
@TiReD - can you remind me of your WAG method going from 'infections today' -> admissions in a week (?) -> deaths (in two weeks)?
What are the false negative rates from the self administer drive through NHS type tests? I was negative last week but seem to be easing my way into some mild form of 'long covid'. Dog walk yesterday left me knackered and with a proper 'brain fog'. I took the wrong turn driving home, which is less than 10 minutes away.
Admissions in 10 days are cases/14. Deaths in 21 days are cases/50. These will change with vaccination. Hopefully that 50 will rise.
Admissions in 10 days are cases/14. Deaths in 21 days are cases/50. These will change with vaccination. Hopefully that 50 will rise.
going by worldometer the peak cases was ~60,000 on the 10th Jan going by the 7 day rolling average. that implies only 1200 deaths a day at the peak at the end of this month. but 21 days ago we were at 40k cases implying only 800 deaths a day now, which seems to be an under estimate, again, 7 day average to roll out the weekend effect.
going by worldometer the peak cases was ~60,000 on the 10th Jan going by the 7 day rolling average. that implies only 1200 deaths a day at the peak at the end of this month. but 21 days ago we were at 40k cases implying only 800 deaths a day now, which seems to be an under estimate, again, 7 day average to roll out the weekend effect.
Might need to used average weekly cases etc I would think.
@TiRed - does you method include mitigation measures?
I would imagine that there be an increasing influence of the lockdown day by day in reducing the transmission, admission numbers. That will be offset by NHS capacity etc.
1,820
I hope Christmas was worth it.
I hope that 1 day of family mixing sending all the kids back to school will be worth it as well.
Perfect time to have a populist as a leader...
But he couldn't have known there was a more transmissible variant going around.....oh no, wait, he did.
Almost wish I did Twitter to share those posts
Do you think Boris cares at all that people WILL have died today because of his narcissistic will to not be the PM who took away Xmas.
Because I don't think he does.
Otherwise he wouldn't have done it...
He thinks it makes him look strong. It makes him look so so so weak
Almost wish I did Twitter to share those posts
I left the platform as mental health went downhill rapidly just before Christmas. I'd recommend staying well away MCTD.
I think that’s wise advice.
I left the platform as mental health went downhill rapidly just before Christmas. I’d recommend staying well away MCTD.
I'm just about hanging on with Facebook
I got rid of Facebook a few weeks after lockdown 1....one of my better decisions recently. I miss the gear exchange pages and the ground conditions page....that's it.
I'm pleased to see there are some areas of blue re-emerging amongst the red where I am on the Southern fringe of Greater Manchester.
https://coronavirus.data.gov.uk/details/interactive-map
while in other news
Police have urged people not to "drive to see the floods" as evacuations of households in the wake of Storm Christoph begin in England and Wales.
https://www.bbc.co.uk/news/uk-55743246
Wot??
Neutralising ability of antibodies typically falls eight-fold with South African variant
If this turns out to be true, are we back to the lockdown vs herd immunity argument? This seems like a policy failure if the vaccine deployment can’t keep pace with the not only global demand but also the rate mutations.
Unless we start looking at this through the effort and timescale required to finish world war two, I’m beginning to wonder whether we’re either fighting a losing battle or in danger of the medical public health equivalent of getting bogged down in Vietnam with ever increasing mission creep.
Any of my university years would have been worst. I can put my life on hold right now, but the uni years were the best and hardest of my life, I’m not sure I could have coped with that at that age, knowing it could never be undone.
University was four years of getting high as **** and playing Fifa with complete degenerates.
It would have been exactly the same with Covid going on, as the students living in the accommodation next to my apartment can seemingly attest to.
University was four years of getting high as **** and playing Fifa with complete degenerates.It would have been exactly the same with Covid going on, as the students living in the accommodation next to my apartment can seemingly attest to.
Four years of travelling around riding bikes and going out for beers would have been fairly badly affected. Selfishly I'm very, very glad this didn't happen when I was a student.
Also a very bad time to be a graduate, as my two cousins will attest to. Imagine trying to find your first graduate job just now...
If this turns out to be true, are we back to the lockdown vs herd immunity argument? This seems like a policy failure if the vaccine deployment can’t keep pace with the not only global demand but also the rate mutations.
This is my worry, we can't keep on locking down year after year, when will it ever end?
International travel will open up eventually, so these variants will freely circulate the world at some point in the medium term and then mutate again and again.
Not exactly an exciting future to look forward to if so, being re-jabbed for new variants and lockdowns to manage them prior to rollouts?
If this turns out to be true, are we back to the lockdown vs herd immunity argument? This seems like a policy failure if the vaccine deployment can’t keep pace with the not only global demand but also the rate mutations.
Surely the key question is about the severity of the disease that would result from the SA (or another) variant in someone who had either been vaccinated or infected. For the current variants the emerging picture seems to be that a second occurrence is generally less severe than the first, so if new versions of Covid end up being very transmissable but generally don't causing severe illness then it starts to look a lot more like the flu which doesn't require such strict measures. If it goes the other way then we've got some big decisions to take as a species.
Neutralising ability of antibodies typically falls eight-fold with South African variant
We need to scout around the genomes, find the best transmitting but vaccine compliant uber-variant and lob it into SA and wherever to duke it out with their variant. Last virus standing wins. 🙂
It's likely the vaccine will have to be tweaked sooner rather than later, then probably tweaked again. It's the way of the world until this coronavirus has circled the globe a few times and lost some of its underlying novelty.
Vaccination is the short-term solution for total lockdown, the medium term solution for partial lockdown, and the long-term solution for protecting the most vulnerable year on year.
I seem to recall TiRed and others have been saying from quite early on the new variants will probably reduce the severity, vaccination may need to be annual thing with updates perhaps, and eventually this will become similar to flu interns of its effect on public health.
This shouldn't really be surprise.
But there will be a new normal - masks and hand hygiene will become more commonplace - I hope, suspect a lot of people will be more cautious around distancing, international travel isn't going to open up in the same way for quite some time.
Admissions in 10 days are cases/14. Deaths in 21 days are cases/50. These will change with vaccination.
Could add
Cases in 10 days are turkey dinners/1000
As the virus is already transmittable asymptomatically, the evolutionary pressure to become less harmful presumably isn’t that great. I wouldn’t plan based on that happening over the next 18 months, that’s for sure.
We need to wake up to the idea of containing and starving the virus of hosts, not just using social measures and partial vaccine rollout to try and prevent hospitals being full of Covid patients.
In case folk are not sufficiently depressed, seems that the new variant may be spreading too fast to cope with via lockdowns 🙁
As the virus is already transmittable asymptomatically, the evolutionary pressure to become less harmful presumably isn’t that great. I wouldn’t plan based on that happening over the next 18 months, that’s for sure.
Agreed. This is what I have been quietly worrying about, there are a lot of people in my industry (pharma) who are saying “oh it will be alright, the new variants will have reduced severity”. Only 10 percent of the population is confirmed to have had it, we already have 100k dead and the evolutionary pressure to mutate into a less severe form is simply not there. If the new variants are that good at avoiding the immune system I think they’ll even cause significant clinical disease in those who have already caught the virus before.