Forum menu
Interesting article on vaccine priority lists and current government direction.
It looks like age related, going down in 5 year jumps from 80, with care homes and their workers first and more general "health and social care workers" next highest.
Can I ask the experts, is 90% good for vaccine effectiveness?
And is that 90% likely to be repeatable in the older or more at risk population, do vaccines work well for everyone because we are all basically the same, or are we likely to see significantly less than 90 because the vaccine can't provoke immunity as well in less strong immune systems?
Looking at the other way round, 10% failure in a group like the over 80s is a lot more dangerous for them than it is for the type of person likely to have been in the trial. I'm assuming they are healthy youngsters usually?
I understand that at a population level, eventually, vaccines work by massively reducing the chance of being infected, so I'm not asking about that- more about individuals biology and vaccine response.
And can anyone expand on this bit from the BBC article:
There will also be some people - such as those with a weak immune system - who will not be able to have the vaccine.
https://www.bbc.co.uk/news/explainers-54880084
I met someone late summer who's job was writing drug trial proposals.
She said alot of testing was established drugs being tested to see if they had any effect and any likely vaccine would end up using existing drugs (I don't know the exact term compound? Ingredients?).
She worked for a decent sized phama company.
Seem a plausable first step.
The 90% number is just a wild guess at this point. There is huge uncertainty. It would be useful if achieved in the broader population (and just about anything is better than nothing - flu jab is generally reckoned to be about 60% effective and we haven't had a bad flu year since it's been introduced AIUI). Some vaccinations are (well?) over 95% effective though, which may be necessary to really suppress it long-term depending on take-up.
From reading between the lines, the 90% figure in the publicity was probably derived from a trivial calculation like this:
Two equal-sized groups of people, half got the vaccine, half did not.
86 of the non-vaccinated people got ill (entirely by chance)
8 of the vaccinated people got it.
Assuming that 86 of the vaccinated people would also have got ill if they had not got the injection, we estimate 86-8 = 78 infections were prevented in the latter group. 78/86 = 90%.
The uncertainties on such a calculation are large, it's just a first estimate, and there is no indication of the durability of the immunity.
My prediction is the final answer will be rather lower, for a number of reasons. But it might still be useful, and there will be other vaccines.
Which conspiracy theory will be strongest next year? One of the “anti-vaccine” ones, or one of the “they’re deliberately denying us mass vaccination” ones? Place your bets now…
The one I have heard manages to combine both. They* are prioritising giving the vaccine to old/vulnerable people to kill them off. Proven because someone's 93 year old nan got the flu jab and was dead within the year. It's quite a nasty and insidious one as it can be defended on the basis of concern for others. As with many conspiracy theories the proponents are usually unclear on the question of "Why?".
*They can be any or all of the Government, Bill Gates, George Soros, the Village People, Lizard People etc.
There will also be some people – such as those with a weak immune system – who will not be able to have the vaccine.
Passive protection from antibodies will be available.
From reading between the lines, the 90% figure in the publicity was probably derived from a trivial calculation like this:
Welcome to the world of drug development. Pivotal trial analyses are almost invariably “non-parametric”, ie assumption-free. An exact test for difference of proportions is a chi square test. This is normal and necessarily conservative from a regulatory perspective.
As for 90%, well if is about 9/10 after 28 days. Let’s see what it looks like at six months. Over 50% would be a good outcome. I’m serious; 1 - (9/10)^6 would be at least 43% still protected.
So this vaccine is going to require two carefully spaced doses and take about a month to become effective. It will probably be time limited and require regular booster doses.
It needs to be rolled out to 10s of millions across three countries who can't agree on a common plan by a government that has a less than stellar track record in controlling the pandemic.
Its recipients are a population where a significant proportion are fed up with/don't follow/ don't understand the rules and where most just want to return to pre-Covid normal.
What could possibly go wrong?
Anyone know the CI on the Pfizer 90% number? I'm struggling to track down the paper (anyone got a link?)!
There is a definite correlation between Brexit (sorry but it’s what ive seen), anti mask, pro Trump, anti lock down and anti vaccine.
Hardly a conclusive study but I think others will say they might have observed some of the same?
There's definitely a link, though I'm proud(?) to say my Brexity brother in law was kicking off at an anti-masker on FB the other day. Admittedly, suggesting people refusing to wear a mask without a medical reason should be shot did leave him open to the accusation of being a Nazi. On the other hand, it's a much swifter and more focused application of Darwin's Law, without the risk that the anti-masker will survive Covid but infect and kill my granny. It's worth serious consideration maybe. 🤔
Luckily we already have processes in place for mass seasonal vaccination for flu. The cold chain will be new but providing the government stays out of the way I've got no doubt "big pharma" and the NHS can handle it.
So we're screwed.
There is research that suggests certain people are more prone to conspiracy theories in general so it's not unreasonable that the Venn diagram of Cv19 deniers, antimaskers, brexit loons and antivaxxers would have significant overlap.
Who believes in conspiracy theories?
Also remember that there is no problem for conspiracy theorists believing in several mutually exclusive theories at the same time. E.g. CV19 was created in a lab to kill everyone but CV19 is just the flu and lockdown is a waste of time. The government is incompetent and has messed up the handling of Cv19 but CV19 is a careful designed government plot to systematically murder the elderly.
Go on then I will say it, any conspiracy theorists I know tend to be a bit thick (that is the common denominator)
Thanks @thecaptain and @Tired
So practically, it is likely to improve the survival chances of an elderly relative in their 70s, but it's not a magic wand replacement for careful hygiene, reduced contact and mask wearing.
And for someone immunosuppressed from chemotherapy - not really a proven alternative to shielding yet, but wait and see.
?
And for someone immunosuppressed from chemotherapy – not really a proven alternative to shielding yet, but wait and see.
Indeed. This won't work for mrs_OAB's condition, no point in her having the vaccine, yet she is super high risk.
Is an antibody treatment an alternative for an immunosuppressed person?
Anyone know the CI on the Pfizer 90% number? I’m struggling to track down the paper (anyone got a link?)!
Assuming the split is 8/19477 vs. 86/19477 (38954 evaluable after two doses and 28 days - press release said 38955), then the proportions are 0.0004 vs. 0.0044 = -0.0040 (95% CI 0.0030, 0.0050), odds ratio is 10.793 (95% CI 5.229, 22.279), you are nearly 11x more likely to be infected after 28 days if you did not have the active vaccine.
Press releases prefer P values, so that is P < 0.0001, which means that the probability of achieving a split of 8/86 heads/tails for an unbiased coin flipped 94 times is less than 1/10,000. Rather unlikely that the effect is by chance.
BTW there won't be a paper, the analysis will have been done by a statistician on the Data Monitoring Committee yesterday, and the numbers read off directly and released. The SAS code will have been:
data pfizer;
input Treatment Response Number;
cards;
1 1 86
1 0 19391
2 1 8
2 0 19469
run;proc freq data=pfizer order=data;
weight Number;
tables Treatment*Response / chisq exact relrisk riskdiff;
run;
Luckily we already have processes in place for mass seasonal vaccination for flu. The cold chain will be new but providing the government stays out of the way I’ve got no doubt “big pharma” and the NHS can handle it.
So we’re screwed.
I'm pretty confident, NHS locally at least have been planning for months for it. As Tired has being saying, almost no cost is too expensive so Obvs the Gov, BMJ etc will want to argue a bit about who's going to get the millions of pounds on offer for do their part etc, and I'm sure a few isolated issues will cause some sensationalist headlines in the months to come, but the NHS are in no mood to **** about.
Now... if someone could stick Zuckerberg on a ****ing lead before the bullshit starts to fly, we might just be able to see an end to this whole shit show.
P-Jay - my apologies, it was my poor attempt at humour.
Worth mentioning there are two conceptually distinct ways in which the vaccine protects.
1) Direct effect, say it cuts your personal risk of catching the disease by 90%, this number may not be uniform across groups so could have a greater or lesser effect on deaths depending on whether elderly are better or worse protected. Only applies to people who get the injection of course.
2) Indirect effect due to herd immunity, it may suppress the virus (perhaps in conjunction with some social distancing etc). Even those who don't have the injection are protected by this mechanism but if there are too many of them, it won't happen!
Immunising the elderly, as we do with flu, is just aiming at 1 and not really attempting 2. Though any reduction in at-risk population will help to cut transmission a bit.
P-Jay – my apologies, it was my poor attempt at humour.
Oh I wasn't offended mate, and there's ample scope for the Government to **** it up for the sake of giving their mates a big pile of cash. We may well be screwed ha ha.
If GPs want to be on the front line for it, they certainly should be, but I'd argue they're perhaps not best placed to complete the sorts of numbers needed, even at the furious pace they can work under usually.
I think the plan locally at least is to make use of the current testing facilities, you'll be assigned a time slot, arrive as best as possible as a household, be given the vaccine and then wait under the gaze of a nurse in case of an adverse reaction (this is normal for vaccines). I doubt there will be much of a chance to pre-book your slot, it would cause too much stress and panic as people find sites crash, slots fill up etc, but who the hell is going to say "I can't make it, I'm working that day" or whatever.
Very few people of working age will be getting this vaccine....
Very few people of working age will be getting this vaccine….
Yes, I think a fair bit of perspective has been lost on this vaccine, certainly as far as the initial short term is concerned.
As and when we do get to more large scale vaccination, presumably the fact that it needs two jabs two weeks apart or whatever it is, will mean that some sort of planning/booking/organising will be required.
OK, ordered 40 million doses which since two doses are required for each person that's 20 million. A Pfizer scientist was being interviewed on R4 last night and said that they wouldn't have enough in the short to medium term so the stocks would be distributed pro-rata according to orders. The UK would be likely to get 10 million doses, enough for 5 million.
Here's the UK demographic by age - https://www.statista.com/statistics/281174/uk-population-by-age/ work your way along from the right until you get to five million. There'll be some who won't have it but there's also front line health staff who'll be offered it regardless of age.
I'm 61 so there needs to be about that 40 million doses available before I'd be offered it (assuming the "start with the elderly and move down by five year blocks" scenario).
Im 46 so won't get it at all. Interesting to see that Im expected to fly all around the world every day without it.
Very few people of working age will be getting this vaccine….
THIS one, probably not, certainly not in the first 'wave' especially if there's only enough coming for 5m people. 1m people work in the NHS alone, of which maybe half will be front-line workers, we've got nearly 9m people over 70 too.
That said, assuming it's successful, which seems likely, it won't be the only vaccine. the Oxford vaccine was seemingly a few weeks ahead of this one will likely come soon.
Plus, with almost unlimited demand successful vaccines will have ample opportunity to license production elsewhere. Even with the small margins allowed, it will be something of a gold-rush.
If it worked, as the vaccine is rolled out to the most vulnerable deaths and admissions will fall, which is good for everyone, which will allow restrictions to be slowly lifted and the R rate becomes less of a concern.
It doesn't mean come Christmas we can all go back to licking escalator belts or whatever people do, but barring any **** ups, come Summer, things might seems a lot more normal.
licking escalator belts
LMAO
Tired - thanks for the CI information - interesting stuff!
Pleasure - they may have run Intent To Treat (one dose) on 43,538 subjects (21769/arm). The results barely move.
does it not make economic sense tho to prioritise (after frontline nhs, police, teachers etc) some working people to get the economy cranked back up... even young people so they can carry on their education/lives (and not superspread it to the rest of us!)Very few people of working age will be getting this vaccine….
It might, but they have stated their aim, and it isn't that. Care homes, old age, NHS. then working down to 60+
It might, but they have stated their aim, and it isn’t that. Care homes, old age, NHS. then working down to 60+
Yep..as far as I have read anyone under 50 won't be vaccinated. Basically get the vunerable protected then everyone else is pretty much going to be left to get on with it is the government's plan.
Chap from Oxford was today saying that given we don't know the longer term impact of corona even on healthy folks, this may not be the wisest policy.
does it not make economic sense tho to prioritise (after frontline nhs, police, teachers etc) some working people to get the economy cranked back up… even young people so they can carry on their education/lives (and not superspread it to the rest of us!)
There's probably an argument for that, but Priority 1 is to stop people dying and filling hospitals.
As far as I can see though, they're still aiming to offer it to everyone, we'll just have to wait our turn.
I'd guess by the time they're down to people in their 50s and out of the high risk cat, they'll have a better idea how effective it is medium-term and firm up on the plan. It might just be a case they only offer it free to the over-60s and people with underlying conditions yearly like the flu vax and the rest of us can pay for it if we want, or attempt to eradicate it.
I know people were joking about this earlier in the thread at the time but to have the HEad of the efforts admit this is shocking:
Anyone with an ounce of a brain knew it would happen. Draw your own conclusion.
Sounds suspicious. How could so much money go into a project that could make that big an avoidable mistake? Get that MP that’s supposed to be cracking down on corruption onto it… actually, I’m sure he’s having a good chat to Dido Harding about what went wrong at the highest strategic levels right now…
Immunising the elderly, as we do with flu, is just aiming at 1 and not really attempting 2.
Agreed. We should be looking at teachers, front of house staff in hospitality, public transport passenger facing staff, and shop floor workers. Anyone who’s job it is to deal with loads of people a day. NHS and care staff first though… of course… they not only deal with loads of people a day, but a lot of those people are the most at risk.
Good video from 538
And a 4 day window to bid on £43bn of test contracts. That's insane amounts of money.
Good video from 538
Skimmed it. Just pub politics talk. I’ll wait for the Indy Sage video at the end of the week.
I appreciate pfizer are the competition. But frankly the amounts of profit they are going to make off this vaccine are not acceptable.
it is also going to make it a first world vaccine too.
sadly doesn't surprise me from them either
Is it really only around here that schools are struggling thanks to so many teachers testing positive in the last week or so? Utterly confused to see so little about it anywhere.
One of my teacher friends has hinted (quite strongly) that they're not allowed to talk to the media or post on social media about issues they are having. If they're not allowed to speak about it the story gets supressed.
Her school is currently struggling with 30% of the staff off ill or isolating BTW.
I appreciate pfizer are the competition. But frankly the amounts of profit they are going to make off this vaccine are not acceptable.
it is also going to make it a first world vaccine too.
It's something that doesn't sit well with me either, but I can't see an easy solution. If there's no return on investment for them then it's unlikely we would have a vaccine as quickly as w potentially have.
Surely it makes sense for governments to license the vaccine from Pfizer and start producing it 'locally'. I appreciate it's not going to be cheap to either license or build the infrastructure for production, but when you look at how much the pandemic has cost the economy so far, surely no cost is too much?
Any ideas when will we hear about the Oxford version? I'm assuming the UK government have more of a vested interest in that one, so may be more available. Given I've got asthma I'd like to think I'd qualify for a dose at some point, but I'm not holding my breath.
OK, this is a bit of an emotive subject, but I can’t help but feel that some reticence about having the vaccine is not entirely irrational, given the following statements as reported in the press? Still, long-Covid doesn’t sound fun so I would certainly take it if given the chance.
It uses a completely experimental approach - that involves injecting part of the virus's genetic code - in order to train the immune system.
No vaccine has gone from the drawing board to being proven highly effective in such a short period of time.
I know that AZ and others are going to be selling their vaccine at cost (at least during the pandemic).
Does seem normal for pfizer to profit from most things
Does anyone know how this interacts with various testing?
Will this vaccine or the Oxford one test positive on different SARS-COV19 tests?
Are there any rules or guidelines for hospital admissions if this is the case?
You wouldn’t be shedding virus… no idea about anti-body testing. TiRed is your man.
So, it’s Tuesday… the day where, each week, we get to see the real week on week changes in the data, after a weekend of the media over interpreting the always lower weekend figures… and, again, things aren’t going the right way in England, are they…
Not seen today but yesterday hit 500 admission were lower at around 1.3k rather than 1.5k
So today almost 600 and admissions 1.5k again. Cases and admissions seem to have plateaued though, deaths lagging as expected?
I know that AZ and others are going to be selling their vaccine at cost (at least during the pandemic).
Does seem normal for pfizer to profit from most things.
Could this mean Pfizer have pushed things through too quickly? If they're the only company to not agree to offer it at cost then they have a lot to gain by being first. If they can get ahead of the others and have 4-6 months of being the only player in town and thus charge what they see fit, then drop the price as other options become available what's stopping them cutting a corner or two? I know normally there would be loads of checks and balances to stop this but with everything being pushed through in record time, understandably, right now what's the chance they've missed a step and it hasn't been picked up?
Not wanting to poo-poo their work, especially if it is genuinely a solution we desperately need, but it's the first thing that pops into my head when I read that.
So today almost 600 and admissions 1.5k again. Cases and admissions seem to have plateaued though, deaths lagging as expected?
I can't help but notice that test numbers have levelled out or even slightly dropped though, might help supress the number of confirmed cases slightly. Admission numbers are slightly more encouraging though.
I don't think they will have missed anything, the consequences will be far too high for a mistake like that.
Basically if the vaccine comes out as being dangerous due to missed testing then we will have the current situation for a long time as no one would take any vaccine.
Sadly I just think it is profiteering as normal from them.
Plus I don't think they will be first to market. They have just given an interim readout which being cynical has probably helped them get some more orders. But as I said this is a first world vaccine with it costing £30 a go.
So today almost 600 and admissions 1.5k again. Cases and admissions seem to have plateaued though, deaths lagging as expected?
Deaths by date of death are what really matter - these won't be exceeding 500#.
https://coronavirus.data.gov.uk/details/deaths
A lot of pressure to get a daily bed and death count out, but the 7-day rolling mean is a better measure. Date of death is pretty smooth. I've not seen anything to alarm or reject my previous projections of more than a month ago. Now we have Tiers and lockdowns, things will be heading downwards. North West admissions are already going south.
You wouldn’t be shedding virus… no idea about anti-body testing. TiRed is your man.
If you have been vaccinated, you'll test positive in a lateral flow test for antibodies. If you have a monoclonal antibody as therapy, you may not depending on the lateral flow assay used. The PCR test for virus will not care about whether you've been vaccinated.
#just to bait @thecaptain - actually both projections aren't bad at all given the shifting sands of policy 🙂
I don’t think they will have missed anything, the consequences will be far too high for a mistake like that.
Basically if the vaccine comes out as being dangerous due to missed testing then we will have the current situation for a long time as no one would take any vaccine.
I'm thinking more like the Thalidomide issues, where unknown side-effects may not show up for a few years or more. There's been time for short-term issues to be flagged up but not enough for long-term ones. Absolutely agree that all the pharma companies will be very aware that they have a duty to not cock it up as public opinion on the safety of any drugs has to be very high for it to work.
I’ve not seen anything to alarm or reject my precious projections of more than a month ago.

Agreed. We should be looking at teachers, front of house staff in hospitality, public transport passenger facing staff, and shop floor workers. Anyone who’s job it is to deal with loads of people a day. NHS and care staff first though… of course… they not only deal with loads of people a day, but a lot of those people are the most at risk.
Depending on uptake then a regional approach might also work medically if not politically.
Wipe the virus out in specific areas and make a full lockdown in/out (with the exception of medical who have also been vaccinated)
For me the vaccines are a very different beast to the small molecule drugs.
Vaccines induce the body to do something where drugs have a direct action.
the main concern for a vaccine or anything that affects the immune system is induction of an auto immune response and all that follows from there.
With the numbers being tested any significant incidence would be detected, but yes there will be a lot of hopefully minor adverse events reported.
@stevextc - that's sensible and worked in Australia, helped by the major population centres being widely separated (sorry Albury). Unfortunately we're one of the most densely populated countries in Europe with massive interconnectedness so I can't see that working as well.
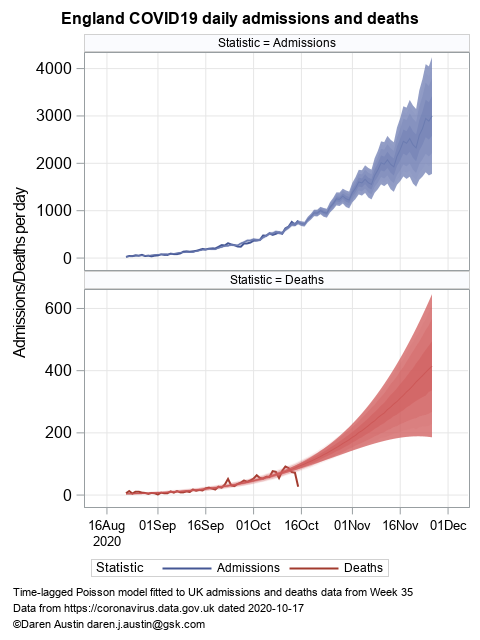
@TiRed, please re-plot your figure of p455 together with the death data that are now available. At a glance it looks like you've massively underestimated reality. I think I hinted at this a few days later on p458...
I wasn't actually going to draw attention to it. But since you insist....
I think 500 deaths/day was the separation, no? (and I mean deaths by day of death rather than the headline figure today). My earlier plots were based only on England data, but since October I've modelled regions and summed to UK. Predicting the nadir and rise looked reasonable, but the precision was poor out beyond four weeks. From November, projection fails due to policy, but I was satisfied with 300 deaths/day by mid-November, rising to approximately 1000 by mid-December in the absence of no policy change. The effect of Tiers will, however, now be pulling down the daily death numbers.
I'm trying to build a model based on ONS survey data and forward projection. This would provide data-driven two-week forward projection.
Not sure what that means @TiRed it looks like a bit of a word salad to me but here is my best attempt to overlay data on your pic:
ok I no longer know how to embed from imgur but the link is here for anyone who wants to check it out.
Feel free to improve my graphic but this prediction was truly awful, no? The tail end where it just pops back in to your dead zone is of course incomplete data.
Or have I misunderstood what that plot was about?
Ah, maybe this will work:

4 weeks ago I said we were on course for about 500 deaths per day by mid-Nov. Admittedly I didn't provide any confidence interval, but that prediction is still looking pretty good to me based on those data up to say 1 Nov. Not clear how much of the subsequent flattening is real vs just incomplete data. There are now clear signs of a slowdown in the epidemic which will feed through into death numbers in due course.
I’m not sure how appropriate Willy waving over a plot of dead people really is. Let’s be careful of the vocabulary and acknowledge the hard work being done avoiding potentially contentious terms.
Murray
@stevextc – that’s sensible and worked in Australia, helped by the major population centres being widely separated (sorry Albury). Unfortunately we’re one of the most densely populated countries in Europe with massive interconnectedness so I can’t see that working as well.
That was without a vaccine though.... I think it would be political...
Ignoring politics then we have the vaccines and resources to start in the M9 corridor and realistically get Scotland Covid free.
Depending how the Irish manage/cope etc. then NI can be done... and Wales .. but just using these "names" shows how politics would interfere.
It might be amusing to see all the "I'm not having a vaccine" people's attitude if they were told "you're not on the list anyway" though. I suspect a lot of switches would occur to "us first"..
@thecaptain - it looks like you're 2 observed data sets are not the same even in late September. If that is correct then you're not comparing apples with apples, more like apples vs quinces.
I think @TiRed's plot was following the trajectory at that time without intervention/mitigation. As we know it's a dynamic system so any prediction 1 month ago won't hold water now due to policy changes Tier 2/3/twelvty etc.
Is it really only around here that schools are struggling thanks to so many teachers testing positive in the last week or so? Utterly confused to see so little about it anywhere.
Nope - our local comp has sent Yr 9 home as they don't have enough teachers to run all years.
They are right on the edge of sending Yr 8 home too.
I’m not sure how appropriate Willy waving over a plot of dead people really is.
No one is willy waving, its called discussion if discussion of important information is surpressed because is hard to hear we are on a slippery slope.
A local secondary school here is on the verge of shutting. Not because they have sick teachers but due to a lack of cleaners to give it a thorough clean every day.
No one is willy waving, its called discussion if discussion of important information is surpressed because is hard to hear we are on a slippery slope.
Well personally I think that accusing people of "word salad" and using expressions like "suppressed" is a little inflammatory, Maybe thats just me and its not my argument have to so I'll back out for the sake of the thread.
Looking back at 455, TiRed's plot is for England and the extrapolation is I assume based on that.
I don't know what thecaptains data is, but an educated guess by comparing to the Gov data here
https://coronavirus.data.gov.uk/details/deaths
on the around 1st Nov point - thecaptain is a bit over 300 and Gov reported 7-day rolling average as ca 320-325 around that period for the UK as a whole
Are you comparing UK to England only?
I still think TiRed's extrapolation has turned out low but maybe not by as much as thecaptain's plot suggests.
No one is willy waving, its called discussion if discussion of important information is surpressed because is hard to hear we are on a slippery slope.
I'm not sure anyone has a problem with discussion, but sometimes the tone and language needs to be considered. I appreciate that we have two people with - to my untrained eye - really useful skills in handling and trying to explain data and trends, but sometimes the tone can come across as two alpha males seeking dominance.
Edit - which distracts from the message
Missed that key last sentence
Tired’s graph specifically referred to the UK, and the slight difference in data sets is because the past few days are always a little incomplete and retrospectively updated, which of course everyone who uses these data sets fully understands. My data are directly off the gov website, deaths by date of death for the UK.
But of course I’m happy to hear his interpretation of the large and rapid divergence.
I was hearing last night of a London primary school where the new demands on the teachers mean that they have lost their non-contact periods, lost 20 minutes of lunch and have more obligatory meetings. The working day there is now 7 till 6.
@thecaptain let me get this right. You're arguing with @TiRed about whose plot/graph is most accurate?
@thecaptain - You're being a bit passive aggressive about this.
The differences start in Sept not the last few days. For those of us who you deem not in the know ( which of course everyone who uses these data sets fully understands.), why don't you explain what each element of your graph represents?
If you worked for me I'd send your graph back to be updated. It's missing series labels. Graphs are supposed to be helping to communicate something so they are necessary whether you like it or not.
I'll go back to what I said many, many months ago ... All models are wrong but some are incredibly useful. You need to clearly articulate why yours is credible rather than just sticking to the "my graph is better than your graph" approach
I’ve just screenshotted tired’s graph, you can go back and look at his description of it but it clearly says it’s UK death data. I’ve just told you what data I plotted on top. It was tired who brought up the subject of how well his prediction had held up. I disagree with his assessment. Hopefully he’ll be along to explain if I’ve misunderstood something.
I acknowledge that debating death predictions can seem distasteful and apologise to anyone offended. But without credible prediction, there can be no understanding or control. And mistaking bad predictions for good is worst of all because it implies a belief in understanding which is mistaken.
It’s a sorry fact that a lot of the prediction from those who claim expertise has been extremely poor from day one of this epidemic. It is clear to me that understanding the details of epidemiology is not enough and that it requires the involvement of scientists who understand forecasting methods, their design and analysis. I am one such scientist. There are many others but most of them already have full time jobs!
I acknowledge that debating death predictions can seem distasteful and apologise to anyone offended.
This needs to be done far wider and frequently for public money/projects.
I've previously speculated they should publish a "cost per life".
An example is say the Channel Tunnel... contractors should submit a financial bid and a deaths projection and then be penalised for every death above the "accepted" number.
I suspect if this was done the tolerance for deaths on similar projects would drop significantly...
We can do the same on completed projects... such as Grenville
was hearing last night of a London primary school where the new demands on the teachers mean that they have lost their non-contact periods, lost 20 minutes of lunch and have more obligatory meetings
In my secondary we have split arrival and depature times split breaks, split lunches, all these need staffing.
I’ve just screenshotted tired’s graph, you can go back and look at his description of it but it clearly says it’s UK death data.
His graph on p455?
It does in the source but the title says England. Which could be lifted from UK admissions and deaths data, but only TiRed knows.
shes saying new liverpool mass test has shown not much covid in Liverpool?????
You're right that is inconsistent I looked at the bottom graph and missed the top title. Later I believe he also said he summed over the 4 nations. The UK deaths time series seems to fit closely to his graphic (apart from the incomplete days) but of course that is quite close to England-only numbers. If his analysis was actually just England, there's still a large mismatch but it would be a bit smaller than on my pic.
But of course I’m happy to hear his interpretation of the large and rapid divergence.
That model was just England data, hence the precision of deaths was low due to the limited data (which isn't a bad description of subsequent outcome). Recent analyses are refined to calculate deaths from admissions (a week earlier). That ties the rates of change together in a more mechanistic manner (like your SEIR model). I also describe NHS regions where the prediction of deaths from admissions is more closely aligned. Then sum all regions to get England and sum countries to get UK. Here one sees a more accurate description (Wales is an outlier due to counting suspected admissions). I still feel very uncomfortable of forward prediction beyond four weeks. That's long enough to see evidence of policy changes. So I consider that fit for purpose.
Expect things to turnover at about half of the April peak in a week or two's time. As for post lockdown - expect stable control in Tier 3, maybe Tier 2 and growth again in Tier 1.