[ I think Hancock has been thrown under the bus by Johnson, Raab and others as regards the EU procurement scheme, and other issues, by the way. ]
“On Monday night, UK firms said they had “no choice” but to keep selling the lifesaving gear abroad because their offers of help had been repeatedly ignored by the Government.”
There seems to be examples of companies switching to PPE manufacturing to help with the crisis, only to have to send it to other countries to make sure it proves useful, rather than clog up their own storage facilities. Better it is used than sits around doing nothing… and helping other countries to either contain or slow the spread of this virus is in everyone’s interest anyway.
https://twitter.com/samcoatessky/status/1252637396497248257?s=21
Whatever. Back to an absence of good government, rather than them choosing to stand apart. Slack rather than dogmatic? Both? Whatever.
>WHO are saying some people don’t produce antibodies
Absence of evidence is not evidence of absence
I should have been more specific....They found serological "testing" didn't show any discernible antibodies (in some patients)
So for the purpose of the discussion absence of evidence is indeed clear evidence that serological testing cannot be entirely relied upon to determine the prevalence of infection in a population (and case aquisition rate). Furthermore it also raises concerns about immunity to repeat infections in some people.
There are different sorts of immune response and it is possible to fight off infections without antibodies.
Does it matter, though? Presumably if the test doesn't show a serological response then what's to say the person has developed any immunity?
Then they fall back into the at risk group and we continue as before.
Nearly everyone I've spoken to who's had a cold in the last ten years is doing the "maybe it was Covid-19 thing". Well, it almost certainly wasn't.
Does it matter, though? Presumably if the test doesn’t show a serological response then what’s to say the person has developed any immunity?
Test QC showed 78/85 confirmed positives via a flow assay of IgM - so it missed 8% of confirmed (PCR) positive patients - that might sound pretty bad at an individual level. But... there are sound Bayesian methods to propagate this uncertainty and still get meaningful data at the population level - I posted an analysis previously of the Stanford trial.
What would be interesting to know is how many of the 78 still have igM antibodies after 3,6,12 months etc.
Interview with Anders Tegnell if anyone is interested
https://www.nature.com/articles/d41586-020-01098-x
Anders Tegnell talks to Nature about the nation’s ‘trust-based’ approach to tackling the pandemic.
delivery from Turkey still on hold https://www.telegraph.co.uk/news/2020/04/21/fiasco-medical-gowns-turkey-emerges-amid-row-ppe/
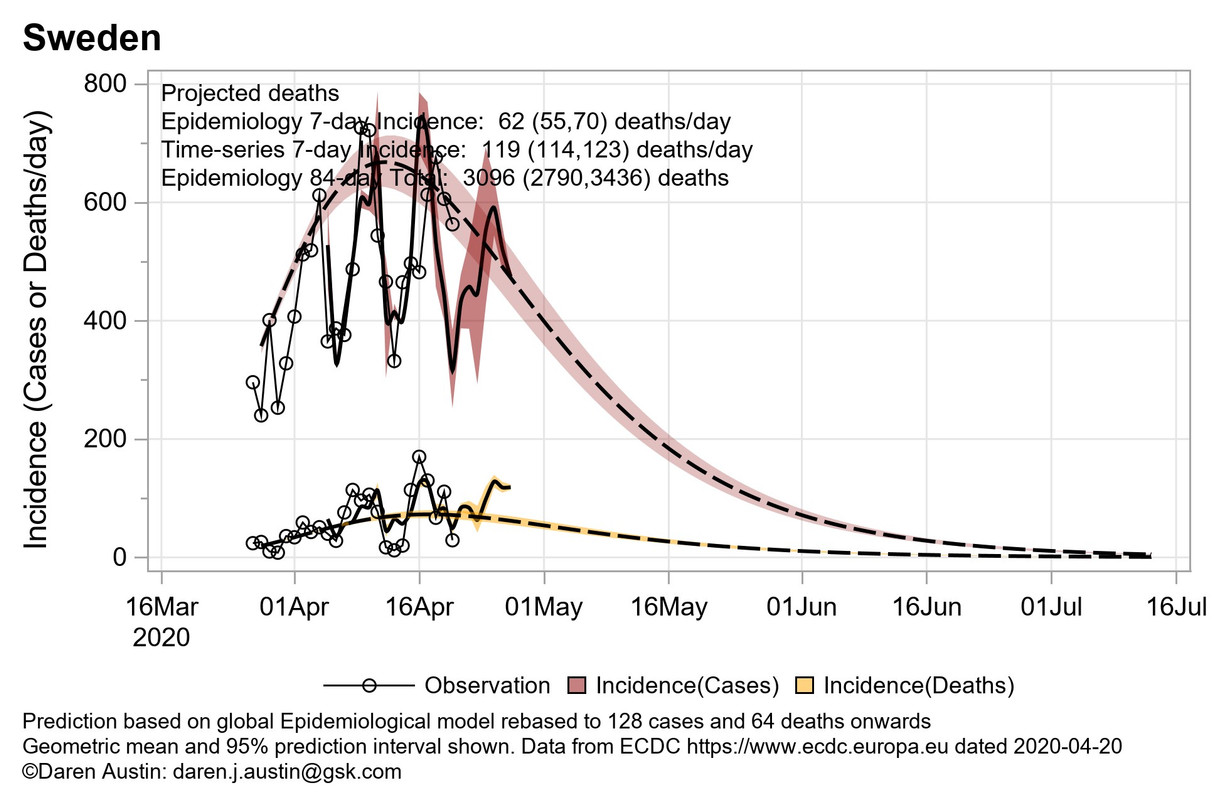
Whilst the numbers are lower, the trajectory and case fatality rate are well-described by the same model as that for the UK and US. I am sure that the more limited social distancing in Sweden is effective, but as I said, they started later, with the benefit of a little hindsight. They are also a smaller country and seem to have the same issues with nursing homes as we do.
Today's data (linear scales)
What would be interesting to know is how many of the 78 still have igM antibodies after 3,6,12 months etc.
well it is a Chinese biotech getting the test out the door ASAP. I imagine that a lot of this nuance will be lost. I've already made one suggestion as to how they might improve sensitivity and specificity, but, like everything in crisis, I imagine they rushed the development, rushed the QC and got it out there as quickly as possible. It's not a great test, but it can do a job.
I'm hopeful for adaptive memory B cells to come to my rescue next year for COVID-20
I’m hopeful for adaptive memory B cells to come to my rescue next year for COVID-20
I was expecting a 19.12 before we get to 20
Is it really likely we’ll get away without a second spike this year?
On the subject of vaccines
What opinions do people have on the risk of rushing vaccines to market and how that balances out against the cost of not rushing?
I’m assuming (as a layman) that you can properly * up a lot of people without proper trials. How do you balance that risk of a lot of people getting *** up with CV19, along with the health consequences of declining economic circumstances.
I can see someone like Trump forcing an insufficiently tested product to market.
Is it really likely we’ll get away without a second spike this year?
I'm no expert, I'm assuming a spike will hit every time we relax restrictions
Maybe Germany is better at hand wadhing than the UK.
A chap on R4 a few weeks ago talking about hand washing at motorway serviced, and influencing peoples actions.
Depending on the day up to 60 % of men didnt wash their hands after using the facilities
The nudge part was using a plant who washed his hands halved the amount of skanks who walked out with out washing
Could be made up for the purpose of radio air time but made me think
If you have a virus that likes being touch transmitted and then uk toilet door handles are perfect for this
Amazing the number of skanky women was also high, 30% soap dodgers.
Well, that’s my take on it Morecash.
I don’t really see the restrictions not being lifted, they’ll come off due to economic and political pressure soon enough. However misguided from a CV19 point of view.
Although the unknown factor is will the transmission behave the same.
E.g. large scale WFH continues where possible, although I can’t imagine I’ll not be unemployed in the next few months.
Germany appears to be experiencing a slight increase in cases a few days after opening up slightly. Need to watch there carefully as they had the most effective lockdown policy of the bigger European states.
I don’t really see the restrictions not being lifted, they’ll come off due to economic and political pressure soon enough. However misguided from a CV19 point of view.
Again, from a position of ignorance, the restrictions are to control the pressure on hospitals, not to eradicate the virus, which will require a vaccine.
Restrictions will be eased a bit at a time to see how infection rates react, but home working and social distancing will remain the norm for most of this year I'd have thought.
Businesses/organisations will have to reopen and operate within social distancing rules as far as possible. People will have to take the risk of catching it however careful they are.
Statistically, the chances of catching it and dying are still low, we need to accept that and try and keep it that way (speaking as a 51 year old overweight bloke, with a wife in a non-ppe key worker role that scares me shirtless, frankly)
Again, from a position of ignorance, the restrictions are to control the pressure on hospitals, not to eradicate the virus, which will require a vaccine.
Exactly, and that could be done by applying some restrictions on those most likely to end up in a bad way with the virus. Yes people under 30 can die from the virus but a lot less likely to and a lot less likely to take an intensive care bed or ventilator.
So let kids out, let least vulnerable out but ensure contact with most vulnerable is limited in same way as now. Don't go to see grandparents, keep social distancing in shops/wear masks in indoor areas where they are other people etc,.
Or you could see how the other countries ahead of us deal with it TBH.
Going by our current success with this I’d see how it plays out before letting loose the hordes on a spreadfest.
I’m pretty cautious about rushing vaccine development. Skipping GLP trials seems remarkable. The publication below teatwd multiple vaccine platforms for the previous SARS-COV-1. They found antibodies were produced. But when challenged with the virus, an immune pathology was generated.
Such studies are not part of GLP toxicology at the moment.
https://pubmed.ncbi.nlm.nih.gov/22536382/?from_term=sars+vaccine+Th2&from_pos=3
Why haven’t the 1600 odd extra deaths up to April 10th outside hospital still not been added to the official tally?
The OFFICIAL tally is always hospital deaths - that is the WHO method of recording deaths, The total deaths is a different matter. 20,000 total is looking aspirational, sub 30,000 would be a success including all deaths.
Reported a couple of days ago, but a nice paper on measuring COVID-19 in water treatment in Paris. Just. Nice. Science.
https://www.medrxiv.org/content/10.1101/2020.04.12.20062679v1
Another study has also been posted online since. I like the orthogonal viewpoint. There are lots of ways of looking at complex problems.
that poo study is great!
I imagine the greater the variety of studies, the wider knowledge we get.
Pooled pooed samples 🙂 . Here's the second study http://medrxiv.org/cgi/content/short/2020.04.15.20066746
This is how you conduct population level sampling - declines here are excellent evidence of population viral burden.
Reported a couple of days ago, but a nice paper on measuring COVID-19 in water treatment in Paris
Wastewater treatment, a subtle but important difference.
Kerley, I fear you are misunderstanding things in much the same way Spain and Italy did early on. We should be learning from their mistakes. You can’t protect the vulnerable without most of the population taking measures to stop the virus spreading. It simply can not be left to those most at risk to protect themselves, we all need to act to protect them by keeping the virus in check (both geographically and numerically).
When the “lock down” (we are not in lock down in the UK) starts to end, it will be paired with continuing and new measures to slow the spread through the “not at risk” in society. We are not two separate communities, the at risk and not at risk… far from it.
that poo study is great!
I'm sure someone will take a dump on it.
If I ever take a piss at the Arndale (in Manchester) I'm always shocked at the number of scrotes who leave the stalls and head directly to the exit without washing their hands. Still, it's possible many were doing drugs...
I attended a conference a few years ago where they posted a researcher as a toilet cleaner to assess hand-washing adherence levels. At the end of the conference they posted the results, that were not exactly stellar. That conference was the Infectious Diseases Society of America, which specializes in infection control. Doctors didn't wash their hands any more than the general population. Not Semmelweis' finest hour!
Always pull the door handle from the bottom when you exit, or dispose of the paper towel outside the toilet.
Not certain of interest to anyone but last year the weekly average death rate was about 9875 (average over 4 weeks in April 2019). Last week we had 18516 deaths (up from 16387 the week before). So approx 8500 people a week extra dying. This would take into account people dying in care homes not currently counted in Gov figures.
I accept it's a rather basic calculation.
I think that kind of study is a load of bollocks; there are very few social situations where you actually 'need' clean hands. The fact that we haven't expired as a species suggests that we can have a wee, even a poo and not die if we don't wash our hands.
How have we managed to evolve for 55 million years given that we've only had sinks and soap for a tiny proportion of that time.
...never mind the whole stickiness of sex and stuff...
How have we managed to evolve for 55 million years given that we’ve only had sinks and soap for a tiny proportion of that time.
with a 50+% child mortality and life expectancy of 30
modern life is rather more, well, long, as a general rule, somewhat coincident with sinks and soap
Which has left us, as a species, somewhat prone to pandemic situations, no?
Always pull the door handle from the bottom when you exit,
What if everyone else has the same idea?
I'm sure game theory could be applied to that.
In an ideal world, washroom doors would open out or there are no doors.
How have we managed to evolve for 55 million years given that we’ve only had sinks and soap for a tiny proportion of that time.
For most of human history, horrible diseases associated with poor sanitation and hygiene were rife though; cholera, diarrhoea, dysentery, hepatitis A, typhoid and polio take your pick.
I'm not suggesting we should lick one another, just that that kind of 'and the Drs didn't wash their hands' study is bollocks.
Which has left us, as a species, somewhat prone to pandemic situations, no?
Pretty sure the human race had pandemics on a fairly regular basis "pre-sink" as well
I had my test the other day arranged by the fire brigade, i was i rag order i barely managed to get back tbh. Results back today and I've got it , ironically I'm feeling slightly better 3 days in,a few from my watch are off with it and even more on other watches but we just cant isolate on a fire engine, unfortunately my mrs works in care homes and mental health wards and now worries that she might have taken the virus in to work but she cant get a test as I've tested positive, ridiculous really loads of tests available but no one can get one hardly, I was the only person at my test center
For most of human history, horrible diseases associated with poor sanitation and hygiene were rife though; cholera, diarrhoea, dysentery, hepatitis A, typhoid and polio take your pick.
Don’t forget the long term offender, The Plague!
‘and the Drs didn’t wash their hands’ study is bollocks.
Google nosocomial infection. It was a simple study for a bit of fun in a population that one might think would have higher hygiene standards.