Forum menu
The media should be sending their science and health correspondents to all media events.
As a health specialist reporter way back when in a previous life, there simply aren't enough of them to do this, and sitting in the no.10 briefing is not a good use of their time, especially as much of the subject matter really is political - economics/policing etc. Tbh they will be more effective working through copy and newswires at base, and shaping the output from there. What we need to do is stop the politics reporters insta-tweeting everything they come across. 🙂
but a thousand
sparrowsstarlings is a murmuration.
Get me an ornithologist, stat!
🙂
So are we now seeing the bounce from the big party weekend 10 days ago?
Or is that still to come?
It’s probably been asked @TiRed but I take it you do stuff like this for a living?
It is used to be my day job, yes. Now I find new medicines at GSK. But the mathematical skills are so complementatry that I have used my day job maths (some mathematical modelling and lots of high-end stats) with my previous epidemiology skills (mainly modelling rather than stats) I used when in the group at Imperial.
If I am honest, I think it has given me a perspective on modelling that I did not previously have in academia. I like to see APPLICATION of my technical work to medicine. And yes, I have invented a medicine that should be launched this year. None of my models ever had that impact. Although you might argue that the Imperial models have (I would not, actually).
PS I'm not a twitcher! Startlings Starlings... damn
Bloody hell, I heard about the French seizing the surgical masks but hadn't followed the details.
The French were concerned that desperately needed surgical masks not be allowed to leave the EU during the crisis. Sweden reluctantly accepted a ban on exports to countries outside the EU, in the mistaken belief that France, like Germany would lift their ban on internal EU transfers, as recommended by the European Commission.
On March 3rd, President Emmanuel Macron announced that he was requisitioning “all stocks and the production of protective masks” for distribution to medical personnel and French people infected with Covid-19.
One fifth of all surgical procedures in the EU use personal protective equipment imported from Asia by the Swedish company Mölnlycke. The company’s main distribution warehouse for southern Europe, Belgium and the Netherlands is in Lyon.
Mölnlycke’s entire stock of an estimated six million masks was seized by the French. All had been contracted for, including a million masks each for France, Italy and Spain. The rest were destined for Belgium, the Netherlands, Portugal and Switzerland, which has special trading status with the EU.
563. Deary me. Quite a jump from two days ago.
Probably bang on track for the fallout, given the incubation delay plus delay until hospitalisation is around ten days, and we are only testing hospitalised cases now.
If you average out the last few days the percentage will likely track steady. I suspect something caused some lag in the numbers.
An anesthetic shortage is the next supply issue according to Europe 1. You can't use ventilators without them and there are not many days of supply left, they're already reusing part-used doses that are normally thrown away as they can't afford to waste the dregs.
If you average out the last few days the percentage will likely track steady. I suspect something caused some lag in the numbers
average % over the last week was 26%, lowest 15%, highest 34%... todays, 31%
oh, and
deaths outside hospitals to be included in UK tally for first time
every tuesday will now include previous weeks 'outside hospital' numbers, so will always be larger
Do we even know what proportion of the ship’s population were tested?
Over 3000 were tested for COVID-19, some more than once.
Mölnlycke’s entire stock of an estimated six million masks was seized by the French. All had been contracted for, including a million masks each for France, Italy and Spain. The rest were destined for Belgium, the Netherlands, Portugal and Switzerland, which has special trading status with the EU.
WTF
PS I’m not a twitcher! Startlings Starlings… damn
You're poorly, we'll let you off - confusion / disorientation is on the symptom bingo.
So are we now seeing the bounce from the big party weekend 10 days ago?
Would that partially explain the lower growth rate in Scotland? (Only 16 today but 547 across the rest of the UK). If so, that might mean some good news to look forward to over the next few days as the effect is replicated.
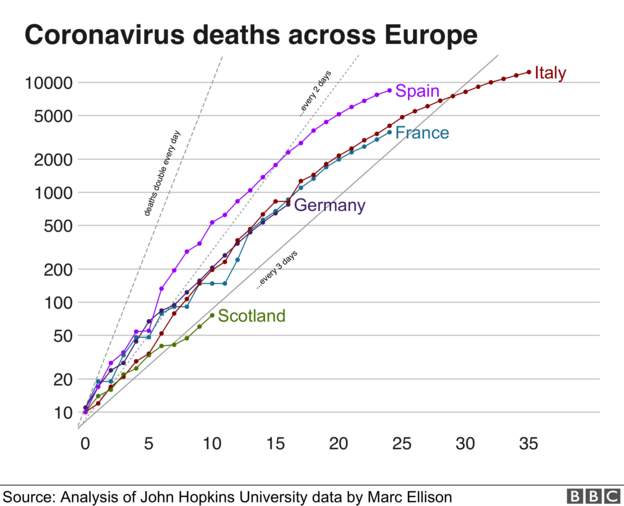
Interesting to see Scotland's numbers being lower. Their population is about a 10th of the others on that graph, which are all very similar.
Wishful thinking - Could it be the beginnings of reaching saturation/a certain amount of herd immunity?
Official cases and deaths still a tiny fraction of population though...
To be lighthearted for a moment... Clearly cabin fever is setting in - our morning meeting this morning.

Wishful thinking – Could it be the beginnings of reaching saturation/a certain amount of herd immunity?
Unlikely. We're nowhere near saturation in any part of the UK. Estimates of % who have 'had it' and who may contribute to herd immunity are in the low single digits. There will be English regions with similar growth rates to Scotland. At the moment the epidemic is being fuelled by London and the West Midlands.
I had a brief flicker of hope when I looked at the drop in numbers over the weekend/Monday, it's only natural, but there's no way any of us is getting off that lightly.
To be lighthearted for a moment…
Am Dram version of The Greatest Showman. Even has Hugh Jackman-a-like...
our morning meeting this morning.
Good work! 🙂
What do you think about the 'models' supposedly used by government medical advisers until rather recently? I believe they were better framed as mathematical conjecture given the paucity of good data? A lot of stock seems to have been put on an old influenza model.
They were the very best available at the time. To describe influenza infection vaccination, treatment and control. That means that the age distributions, mixing behaviours and geographics, validated with decades of data are very sound.
Apply that to a situation where the incubation period, is largely unknown, the transmissibility is largely unknown and the population immunity essentially nil, and see what you predict. Try a range of assumptions and what is the range of outcomes?
When every plausible outcome is bad, advise to act. Forget the headline death toll, this number is nonsense - it's 200,000 (range 2,000 - 2,000,000 - MADE UP BTW). But if the speed of new cases hospitalised cases likely to double every 3 days and you have N (already full ITU beds), then it's a simple model that says you will be swamped in D = log(2)/(N/N(0)) days.
Then you act...
My models are data-fitting and my predictions get better as more cases and deaths accrue. They are statistical-epidemiological models The influenza model has a headstart because it is a mechanistic model with some of the key elements already well characterised. Calibrating it to the COVID-19 is, however more challenging.
Serious wobble myself last night. Shortness of breath, tingling fingers, weakness in arms, muscle pain. The Covid action plan is:
Thanks for the useful posts generally @TiRed. More specifially, just wondering, is the tingling fingers thing a recognised COVID symptom. I had the same thing as well as some weird peripheral vision blurring stuff and had half forgotten the tingling. There's a full run-down of what I've had on the other thread. No test, so no idea if it is or isn't COVID-19, but the impact on my HRV, HR, breathing etc is real and measured.
Rest up and get well soon 🙂
Interesting to see Scotland’s numbers being lower. Their population is about a 10th of the others on that graph, which are all very similar.
Wishful thinking – Could it be the beginnings of reaching saturation/a certain amount of herd immunity?
That conjecture ignores that, where it could, the Scottish government acted before the UK government to stop the spread, as did NI.
Time to bin the ‘herd immunity’ nonsense. This virus needs to be denied new carriers via containment, ‘till we are ready to deal with it via drugs and/or vaccination.
A good friend of mine has just had confirmation of his Covid test - his wife ended up in hospital after a bit of a panic attack due to her breathlessness - He reckons the only symptom he had was a banging headache for one day.
Tbf, it might well be that he had no symptoms, and the headache was just, well, a headache.
BWD - those are all symptoms of dyspnoea - shortness of breath and low blood O2. Raised resting HR is also a symptom of body compensating for low O2. Breath harder - I concentrate on breathing out.
COVID-19 is likely to be an infection of the deep lung alveoli (where the entry protein ACE2 is expressed) that reduces surfactant. That disrupts the Physics of O2 diffusion across the lung. So now you know. I suspect if you have more ACE1 than ACE2 you are protected a bit.
Thanks, that mostly makes sense.
Cheers.
I suspect if you have more ACE1 than ACE2 you are protected a bit.
What would determine that, is it a genetic thing? And I guess higher lung capacity might help as well? Very definitely not a scientist here, so sorry if those are obvious points.
They were the very best available at the time
Interesting comment on the original models TiRed. Lots have been critical of their use, accuracy and the government response, but I'm not sure we were in a position to do any better, and presumably any government would have followed the advice it was being given.
Easy for us all to be wiser now with hindsight.
That conjecture ignores that, where it could, the Scottish government acted before the UK government to stop the spread, as did NI.
Yep - that's why I wondered if the lower trend was something we might expect to see in the next few days from the UK figures.
You’d hope so. Our peak should be just behind, and that hopefully means soon. But the fear is that the delayed response allowed too wide a spread across England and Wales… so we’ll have more cases and a higher peak than we might have had. The big question is whether the peak proves to be too big for the (rapidly gearing up) health service to cope. Hopefully not.
None of this can be known, yet.
What would determine that, is it a genetic thing?
Most likely. But if you have LOW blood pressure naturally, dizzy if you stand up fast, low (I do) then this seems a possible predictor. ACE2 lowers blood pressure by converting angiotensin (angio=blood vessel, tensin = tension or constriction). It’s expressed in many tissues including the lung. So the virus can get in. More ACE2, lower natural BP.
ACE inhibitors might just restore activity for people with high BP to levels the same as those with low. So they may not be at risk on treatment.
Lots of “mays” because we don’t really know. Except we know what ACE inhibitors do.
https://en.m.wikipedia.org/wiki/Angiotensin-converting_enzyme_2
How does your model know how many are or have been infected?
Doesn’t need to. One predicts deaths today from past cases, the other assumes a form for death curve from biological principles. The case fatality rate is what we call a nuisance factor. We don’t know it, so you model what you do know. Hint it’s not a standard SEIR model.
His models are following the progression of the deaths, aren’t they?
I probably should have said the number of cases because the death rate would be #case/#deaths?
There are sampled positive cases (the published figures) but also (hypothetical) unsampled and unknown positive cases. Or are you just interested in critical cases which pass through ICU?
I take global data, then model deaths in each country from the numbers of cases in that country. The ratio is the country case fatality rate. Than number is a random effect with a global mean and some county to country variability. It is a stats model of what we can describe. Not an epidemiological model of what we THINK is going on.
It predicted the rise today. BTW
Most likely. But if you have LOW blood pressure naturally, dizzy if you stand up fast, low (I do) then this seems a possible predictor. ACE2 lowers blood pressure by converting angiotensin (angio=blood vessel, tensin = tension or constriction). It’s expressed in many tissues including the lung. So the virus can get in. More ACE2, lower natural BP.
Yes, I get that, the dizziness on sudden standing, though my measured blood pressure is actually towards the upper end of normal, or at least it was last time it was measured.
Thanks again and best wishes for a speedy recovery.
Tired can i just say....
Amazing without doubt the most positive contribution to "this place" barr none.
Aye, from one GSKer* to another, bravo sir.
*merely a lowly mechanical engineer 😂
You're very unlikely to see lower trends in the UK over the next few days/weeks. Maybe in Scotland/Wales/Ireland, but not in England. The population density is soo high in England, we never really had a chance unless we started contact tracing and isolating the sick VERY early on.
^^^^^^Agreed^^^^^^ STW never ceases to amaze.
TIRed - Do you take into account population density and clustering into account in your modelling?
First time UK deaths superior to France?
Lots of French medical staff complaining about lack of ppe etc...
The UK government is unable to tell the truth it seems,
Decathlon have stopped selling their diving mask to the public as they can be converted for hospital use. 30 000 easy breathe masks and 30 000 swimming goggles according to le Parisien. The masks can be converted with a 3D printed kit.
I know these decisions are not alien to any doctor in critical care medicine, the decision where to give care and where to withhold. I guess eg: on arriving at a RTC a decision could have to be made immediately that while A and B could be saved A has a better chance and B has a poor chance so A gets treatment and B takes their chances.
But if it hits the scale threatened this is a different matter entirely.
TJ brought this up a few weeks ago (I think it was TJ) but is this time for that conversation. If someone is beyond help, or deprioritised to the point where they won't get the help they need, does a civilised society leave them waiting or help them away?
If someone is beyond help, or deprioritised to the point where they won’t get the help they need, does a civilised society leave them waiting or help them away?
Large dose of morphine, and take away the oxygen.
My sis is senior ITU nurse, that's what they've been told. Wife used to work in the local hospice, happened there too, it's not anything new.
The UK government is unable to tell the truth it seems,
How surprising, they've always been such a reliable source of excellent well-balanced information in the past....
[img] https://pbs.twimg.com/media/EUJNXKfWsAEa8rY?format=jpg&name=large [/img]