Forum menu
Except for all the kids not taking part in testing due to lack of parental consent.
Tell that to the teachers that risk catching it.
Haven’t you heard? Schools are safe.
Haven’t you heard? Schools are safe.
Reclassify everything as a school and we’re good to go 😉
I suppose safe is a relative term,always had a laugh with the whole meeting people inside, 1.5m distance was it,easier to achieve in a country pile than a housing association flat.
Anyway I’ve more faith in the scientists,chemists etc who are getting us out of this, the politicians well would it really be bad if we put them against the wall this one time 🙂
I'm struggling here with what some of you actual want ? Do you want no schools to go back ? Ever ? Or until what criteria have been filled ?
Not sure who that’s directed at, but schools have never closed. I wanted the use of (and the funding for) blended learning from September, using additional public buildings not just packed schools, and for no child to have been away from school for any extended period of time. We keep going for an “all pupils on school premises 5 days a week” approach, and ending up with half of kids stuck at home for months on end instead.
It’s right that schools should be prioritised over businesses and leisure in terms of staying/being open. But that should have been paired with prioritising schools in terms of mitigations as well… and that meant space and barriers (fewer kids in school buildings, and older kids using masks in classroom settings). Blended learning would have enabled those that had to isolate this last Autumn and Winter to keep up with more of the work they missed as well. But now? What would I want? Two things… no Big Bang return to schools buildings, have only a few years in each day, and then working from home the following day… or alternate weeks. Yes, more work for teachers and a pain for parents and their employers… but that’s what “prioritising schools” means. Second thing, they should have vaccinated school staff three weeks before the “return”.
it's directed at 'people' in this thread, no-one in particular... but many seem to be frothing about school, so i'm asking.... what do you see as the correct process if what the government are doing now is wrong.
Not sure who that’s directed at, but schools have never closed. I wanted the use of (and the funding for) blended learning from September, using additional public buildings not just packed schools, and for no child to have been away from school for any extended period of time. We keep going for an “all pupils on school premises 5 days a week” approach, and ending up with half of kids stuck at home for months on end instead.
It’s how smart you play it, we need everything open in a way that doesn’t continue the boom and bust tactics.
The stats I saw today on school testing uptake were very high. As ^^^ I’m sure some areas will be different.
Kelvins post on school opening all sounds sensible to me. Too late sadly.
Ah should have said ‘you’, I moved countries during COVID and it’s very,very strange as still working from home not only do you forget the days but the country as well.
Not sure how/when I’ll get my COVID shot but on the upside I’ll have a nicer beach for my staycation 🙂
So what does this really mean? There seems a collective sigh of relief at the current rapid drop of deaths and cases, but now we’re to expect a rise again.
A lot of people really do need an attitude adjustment over their behaviour (not aimed at you, obvs). The current round of vaccination is being presented as an endgame, but it's just a step in the arms race. We need to get kids back to school and allow businesses to open, but that can only work if there is heightened vigilance and the type of behaviour which gives us a chance to drive down numbers and reduce the signal to noise ratio so the health authorities can bring resources to bear on the next stage of the battle, which is potential vaccine-evading mutant strains. We know these are coming, and with a third of the adult population vaccinated, but many thousands of others carrying the virus, this is the perfect opportunity for them to emerge.
Here's a little example, tucked away among the 'lineages of interest' - shorthand for 'strains we're worried about', but it shows the problems that the mobility of people could cause.
First identified in late January in Kent (as usual), almost immediately into London, then Edinburgh, then Manchester. Loads of mutations, so its interaction with the vaccine isn't fully understood yet.
Hopefully, once the weather improves, numbers will be reduced enough so that potentially-difficult strains such as this can be tracked and controlled, but we all have a part to play in giving the virus as few opportunities to travel as possible.
Question..
All adults are going to be offered the vaccine by end of July however is the intention to offer all adults a booster every year? Or just the vulnerable groups?
I'd assume they'd probably want to offer everyone, especially if other countries have limitations on travel for those not vaccinated. But if that's the case how would they possibly manage the ongoing rollout? The Herculean effort to get everyone jabbed in 6 months is truly epic, however hardly sustainable on an ongoing basis.
You'd probably only need half number of the jabs you are giving this year as its boosters so only one shot for everyone, plus you have a year to do it rather than 6 months. But even still, how could that possibly be managed without a permanent army of vaccinators in place?
All adults are going to be offered the vaccine by end of July however is the intention to offer all adults a booster every year? Or just the vulnerable groups?
I'd assumed the latter. Do it with the flu jag. Maybe extend the age qualification slightly as they already did this year.
Or hope that we develop a nasal spray that folk can do at home.
An optimistic viewpoint would be that you'd offer at-risk groups a jab on the same basis as the current annual flu vaccination, based on likely-to-be-dominant strains at that point. It depends on the effectiveness and longevity of the vaccine, the ongoing level of mortality and morbidity in other adults, and raw case numbers going into winter. This year I'm hoping they'll get back around the whole adult population in Autumn/early winter this year with the revised vaccine - Novovax is due to come on stream in August/September, I think, so maybe that will be developed with this in mind.
Well, if you’ve now got 10,000 volunteer vaccinators, that’s 6000 people each to vaccinate.
Take out all the social distancing & PPE requirements then it would be a lot quicker.
If a booster campaign started in September I reckon it would be completed by Xmas. Then maybe every 2 years?
I also read that many 2nd gen Covid vaccines are designed to be more resistant to mutation.
One of the experts on the Zoe Webinar stated that there are only so many mutations possible in key parts of the virus whilst maintaining the ability to transmit to humans. This is unlike flu.
Are all the vaccines spike protein based?
Are all the vaccines spike protein based?
No, some are inactivated virus. The first from Sinopharm showed only 50% efficacy, but a more recent one from Sinovax gave a much more impressive 80%. This is for symptomatic infection counts, not hospitalisations and deaths.
One of the experts on the Zoe Webinar stated that there are only so many mutations possible in key parts of the virus whilst maintaining the ability to transmit to humans.
That's true to an extent, but the surface of the spike protein is highly plastic, with more than 500 mutations recorded on the GISAID sequence database. I think that the expert is right in that it is not influenza, but wrong in that the plasticity is enormous whilst still retaining ACE2 engagement.
The next generation vaccines will code for multiple mutations, specifically the immune-evading E484K mutation that escapes the most potent (bit not all) antibodies and defines the SA and Brazil strains. This may be with multiple spike proteins or multiple strands of mRNA.
Sorry to post off the timeline, but going back to "what's next", I'm not buoyed by Chris Witty's interview this morning. Essentially predicting another spike after this release of lockdown, I logically acknowledge that cases may no longer equate to serious illness or death for most, but emotionally I'm quite anxious about the fact that there's yet another spike to manage. I guess we have to learn to live with it but I'm finding it very hard to de-scale "living with C19" to be the same as "living with Flu".
This doesn't really need a response I guess, its just an anxiety driven brain dump.
Perfectly valid concern, but as TiRed has said all along, we will have to learn to manage this the way we learnt to manage flu.
And we are well on the way to that, only 12 months on from the start.
we will have to learn to manage this the way we learnt to manage flu
Yes we will. Some people think that we'll be at that stage this spring. I now doubt we will.
I’d assumed the latter. Do it with the flu jag. Maybe extend the age qualification slightly as they already did this year.
Whilst i agree thats probably what they may do, it kind of negates the point of vaccinating everyone now if they take that approach. Way I see it the virus will be rife in society for years to come. A one off vaccination for non risk groups only pushes health implications for younger folks a year down the line.
A one off vaccination for non risk groups only pushes health implications for younger folks a year down the line.
Why is that? If everyone has had their initial exposure, or vaccination, the assumption is there are likely to be less ill, if at all, if exposed to future variants. Everyone benefits from the two jabs this year, even if they don't have (or need) boost jabs after that. No one knows if we will chose mass boosting, or targeted boosting, yet, anyway. Other countries do mass vaccinations rather than targeted vaccinations for flu already, for example. Wait and see...
Release from lockdown will naturally increase transmission. So cases will rise. But the case mix, the age breakdown of symptomatic infection, will not be the same as last time. The elderly and most at risk will have protection from morbidity, so the rise in hospitalisations will, one hopes, not follow the same past trend.
Now how big is the trade off? Does five times more infections in people who are twenty times less likely to go to hospital, a good strategy? The government is betting that this is the case. And I think it’s reasonable too.
Next winter. Will present a challenge on healthcare as things come back to more normality and influenza decides to return. But this is progress.
Why is that
Because I had assumed immunity from vaccines will be 12 months at max even if no additional variants.
If thats the case, and assuming the virus is still kicking about in 5 years, I'm struggling to see how those who haven't received a booster will be in any way protected?
I think it's clear to a minority that this is far from over. This year is the litmus test of vaccines. The next winter could be just as harsh as what we've just gone through. My anxiety is all over the shop. Some days I'm alright and the next day I'm really quite bad. It's very hard to feel settled these days about what is around the corner.
I really don't think we will be anywhere near normality at the end of June.
and influenza decides to return
Someone (Whitty?) mentioned this the other day: next winter's flu season.
After we've spent 18 months hiding indoors our herd flu immunity is going to be down.
On the other hand, will some sort of (inherent, if not mandated) social distancing and better use of basic hygiene reduce flu transmission?
I’m struggling to see how those who haven’t received a booster will be in any way protected?
Because it won't be as a first exposure. They are likely to get less ill, if they get ill at all.
I really don’t think we will be anywhere near normality at the end of June.
No, but we will be a much better situation over the summer than we are now. We'll be meeting up for rides, and drinks with mates in beer gardens... even if many of us are still avoiding queuing indoors for things we can well do without. Not back to normal, but with much more in our lives than just our work and homes lives. Tough time for many businesses still. Better times for seeing people and getting out of our heads*.
[ *not like that ]
Because it won’t be as a first exposure. They are likely to get less ill, if they get ill at all.
Even after a lengthy period of time? Everything ive ever read about the vaccines suggest that there is a limit set on how long protection lasts for.
So in 12 months you may have good protection, less so after 24, and after 3 years you'd have none whatsoever.
Perhaps tired can give us his thoughts.
Conjecture... it all depends now what you mean by "protection"... time will tell. Hoping for less severe illness, but not expecting either no illness, or assuming significantly lower transmission, after a long period without a booster... seems the way to go into planning/deciding if/who/when to do boosters. How those boosters perform in tests will also inform how we use them. I'd guess at everyone who wants to being given a booster year one... and then a decision being made about whether to drop to targeting groups in following year... probably the elderly and medical and care staff... maybe young adults.... who knows this far out? No-one.
So in 12 months you may have good protection, less so after 24, and after 3 years you’d have none whatsoever.
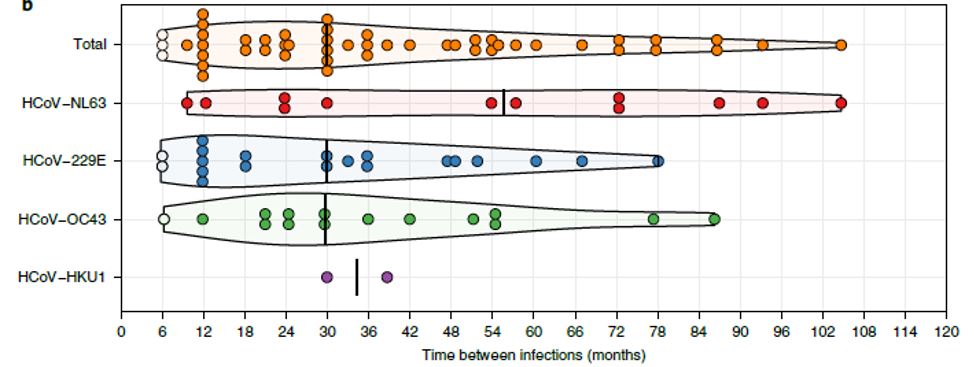
Average time between endemic coronavirus infections is 30 months. So very much this I am afraid. Animals do not live long enough for waning protection to be a thing. Hence we will see booster vaccinations, tied in with influenza vaccination.
"Protection" is really measured by hospitalisations. That burden has been hugely reduced in trials. But duration of that protection is unknown. This is the first cycle really, we are nowhere near endemic, seasonal infection.
This is the first cycle really, we are nowhere near endemic, seasonal infection.
Can you push that comment towards someone who can should it loudly, please?
I believe Witty is on message 😉
This is the period between infections of the four endemic coronaviruses. Line is median
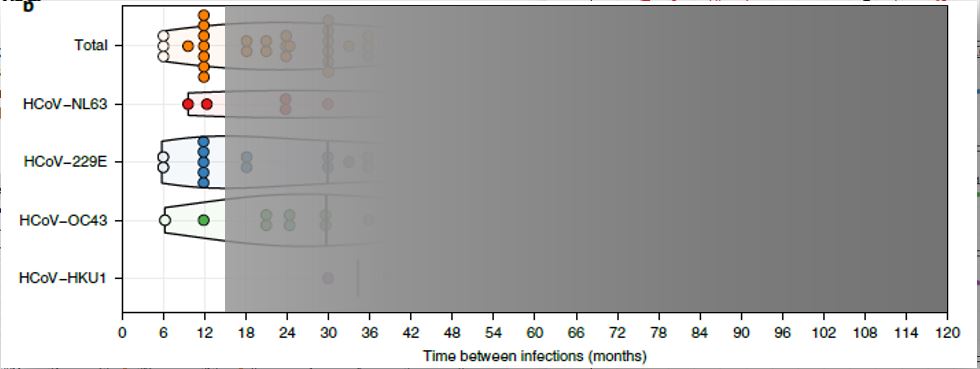
This is SARS-CoV-2
After we’ve spent 18 months hiding indoors our herd flu immunity is going to be down.
Will it? It seems immunity to a particular strain can last your entire lifetime. For example a recent seasonal flu was very similar to the Spanish flu and people who had survived the Spanish flu were immune to that particular strain. Also this study showed that survivors of the Spanish flu still had their immunity to a reconstructed Spanish flu virus almost a lifetime later http://content.time.com/time/health/article/0,8599,1835907,00.html
Two things - does each circle represent a number in the graph above @TiRed? If so, what?
Also, wrt Influenza, this is an interesting infographic -

Each dot is one infection data point. There were 10 subjects followed for up to 35 years with serial serology. So across the four viruses people tended to be reinfected about every two and a half years, but with a long tail. I can’t see why this coronavirus will be any different, other than we can boost immunity if we have to between infections. With an annual or biannual vaccine.
Mrs Tired has her appointment. She’s 51, I’m still waiting. Perhaps they sorted ascending not descending age.
So based on that we can expect a big C19 issue around 6, 12 & 15 months time then, which coincides with Flu seasons 2022 & 2223 respectively, with Lockdown easing contributing to the first also. So pretty much the waves as we've experienced so far repeated for several years mitigated by preventative measures.
Kryton that would be without intervention - ie vaccine. So with updated boosters we can avoid another wave.
Is it possible to vaccinate at the same time with the C19 jab and which ever flu is prevalent in that particular season? (in the future). In other words 2 during the same appointment.
Edit - without lessening the effects of the 2 different vaccines (sorry I'm not being very articulate).
This is the Last Chance Saloon for restrictions, isn't it? I can't see there being any widespread public support for another tightening up, regardless of infection/death rates.
time with the C19 jab and which ever flu is prevalent in that particular season? (in the future). In other words 2 during the same appointment.
They are looking into a combined jab already so it must be feasible. Obviously the big issue there is under 50s don't currently get offered the flu jab, but assuming you can do both jabs at same time it would certainly massively cut down on additional resources required.
Certainly good for me if they did that, I'm eligible for flu jab but not the covid one!
Whilst i agree thats probably what they may do, it kind of negates the point of vaccinating everyone now if they take that approach.
Part of the point of mass vaccination in adults is to reduce the number of people in whom the virus is circulating over the next six months. Each one of those represents opportunities for the virus to mutate, and thereby the chance of producing a vaccine evading strain even sooner.
Next winter will be challenging, without a doubt, but even more so if these strains are popping up too regularly to incorporate into a booster for the vulnerable.
Obviously, we are also vulnerable to imported strains, which is why a mass exodus abroad this summer isn't necessarily the best idea.
Our performance this year is key to the kind of winter we're going to experience going into next year.
Each one of those represents opportunities for the virus to mutate, and thereby the chance of producing a vaccine evading strain even sooner.
Rate of mutation within an infection is a lot higher than people think. In the Lilly studies of symptomatic infection, about 1% of patients developed E484K mutants DURING their infection on placebo (so untreated). And 22% had persistent high viral load. So hope they don't spread... For antibody treatment it was >10% due to selection pressure.
Table 8. This is a highly plastic virus, but cross-reactivity is tending to keep it in check.
Test and Trace is coming in for a kicking today.
Especially worrying is the description of it having "No clear impact" on infection rates and the lack of people contacted actually respecting the isolation periods.
I must not have been paying attention with regards to the t&t situation as when I saw the amount i assumed it would have cost quite abit more than 37 mil
Then I reread the figure...and almost fell off my seat. That's almost 750 quid per every adult in uk...
Where has that cash gone to??
It doesn't even cover Scotland. I've not seen any costs for the Scottish version but I'll bet its nowhere near 1/10th of that.
"Then I reread the figure…and almost fell off my seat. That’s almost 750 quid per every adult in uk…
Where has that cash gone to??"
Most of the spend has been on "Test" not "Trace". The UK has done close to 100m tests to date - more than twice as much as Germany. That's reagents, systems, sample collection staff, lab staff, lab premises, lab equipment, logistics etc etc.
That said, I think the headline £37B is a budget for two years rather than actual spend to date.