UPDATE: Reviews section refreshed, redesigned, searchable: Go take a look
So do you accept that the 10bn figure is bollocks yet?
also nice graph, apat from the cost whats it telling me? Health Care spending is increasing. Nice to know, so long as the economy grows it's a good thing.
As defence spending is also steadily increasing despite moving from a very expensive cold war into more peaceful times can the UK cope with the role it wishes to play in the world.
Well that is a myth, the fith largest spend in the world just behind Russia, having offensive capability has only made situations worse, Iraq, Afghanistan, libya are all operations that have caused a shit storm, destabilising the region has not helped.
Is it having the capability or the way it went down made it worse? You can have the capacility and do some good with it, for instance sending a UN force of peace keepers to the Isreal/Palestine border to enforece some UN rules would be a very good thing.
Great discussion, we really have a wealth of knowledge here. Some really interesting and insightful posts from people in the industry. The point from bigeared abdout IT and the fact that seperating the nhs into trusts, which was lauded as a progression to save money has actually ending up increasing costs. These are things which can be amended with correct governance.
What about in welfare, any cuts we can make there?
save pensions, pay people what they're owed after paying in all their lives I reckon.
Ooh, are we off posting meaningless graphs again?
Here's mine - it's from a BBC website :
[img] 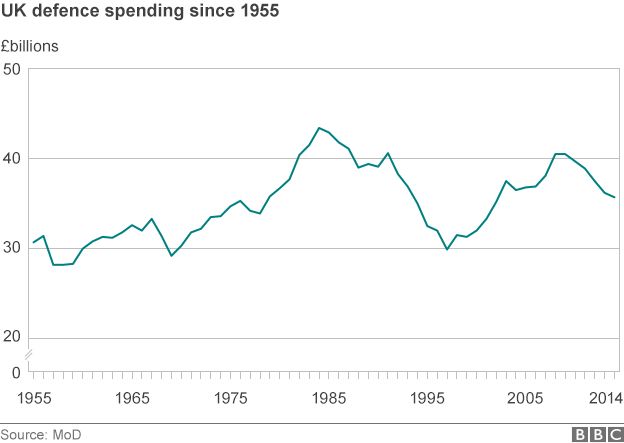 [/img]
[/img]
And here's another one also from the BBC
[img]  [/img]
[/img]
What about in welfare, any cuts we can make there?
save pensions, pay people what they're owed after paying in all their lives I reckon.
I think the consensus was a cull of other people. Back to the so long as I'm good, sure I must be taking more than I pay in mate.
jambalaya - MemberThe Tories have promised to deliver an extra £10bn
What's the exchange rate between a promised pound and a delivered one?
Tom_W1987 - Member
Hi Tom,
again, we weren't talking about climate change: you made the assertion that there is no proof that courses of antibiotics longer than current NHS pot-luck guidelines have any effect on Lyme, and that their supposed over-use by these patients diminishes the overall effectiveness of these medicines.Here is a list of 700 peer reviewed medical papers that all support the claim that tick-borne diseases can persist and survive short term antibiotic use, all state the need for further research and large-scale sample groups:
Please show me just one paper that states Lyme is comprehensively cured by a sub-30 day course of antibiotics, and can prove that longer term use is unnecessary. If you can't do that, perhaps better to wind your neck in when talking about a subject you appear to know very little about. Just goes to show, all you need is one shit in the wrong woodpile and the whole house starts to stink.
Bwhahahahahahah.
None, I repeat none of those papers support the CLINICAL effectiveness of long term antibiotic therapy in humans. These studies have been done.
eg 1200 patients, well designed study, published in the New England Journal of Medicine?
http://www.nejm.org/doi/full/10.1056/NEJMoa1505425#t=article
Hmmmmm. Who do I believe, biased lobbying group or a study in the NEJM? A bunch of papers indirectly supporting a treatment and a good clinical trial?
Tom, for all the bluster show, you're using one study that took 3 sample groups and treated them over 14 weeks. 3.5 months, using two antibiotics that have not and never have been proven to address persistent Lyme infection, and which doesn't mention patients possible coinfections with other tick-borne organisms such as Babesia or Bartonella, both of which impair the successful treatment of Lyme through the suppression of the immune system. Hardly conclusive proof of anything other than their inability to design a better trial.
That paper is so flawed it would be like me taking three faulty washing machines and trying to fix them using a random assortment of tools used to fix lawnmowers then saying "I couldn't do it in 30 minutes so they're obviously broken" Can you imagine anyone saying "I couldn't cure your HIV in 14 weeks with two drugs so sorry, there's just no benefit to treating you further or doing any more research'? It demands money that isn't being spent to establish why Lyme turns into a chronic illness in some people, and unfortunately there's too many over-opinionated assholes like you that either don't want or are unable to acknowledge the lack of science underpinning current policy and any emerging research that contradicts you.
If you cared to look at more recent articles on Lyme you'd see that even the man who designed current US Lyme treatment protocols admits he got it wrong on the bacteria being able to persist, and that their ability to alternate between blood-borne and cystic forms renders antibiotics between 60 to 1000 times less effective as a result. Does that mean long term antibiotic use is the solution? Perhaps not, but until actual research is done to establish what treatment is effective in chronic lyme cases then we won't know, will we?
This article-published today-sums up the bias of arrogant tools like you quite well, but don't let that stop you being a snarky **** whatever you do... Sincerely, my deepest hope for you is that you reap your own reward and get to deal with the kafkaesque process of being diagnosed and treated for Lyme-it might cultivate some humility alongside the bacteria.
Tom_W1987 - MemberBwhahahahahahah.
Actually, if you care to read the comments on your own cited paper-from an assortment of scientists and doctors around the globe-they spell out quite clearly the flaws in the study, from the failure to account for the morphological nature of the bacteria, co-infections and also, that their own results showed that despite improper administration of IV antibiotics for a period shorter than the life of the bacteria, that there was... a mean improvement in all test groups after the 14 weeks. Too bad they attribute that to a placebo effect.
http://www.nejm.org/doi/full/10.1056/NEJMoa1505425#t=comments
.
Tom, for all the bluster show, you're using one study that took 3 sample groups and treated them over 14 weeks. 3.5 months, using two antibiotics that have not and never have been proven to address persistent Lyme infection, and which doesn't mention patients possible coinfections with other tick-borne organisms such as Babesia or Bartonella, both of which impair the successful treatment of Lyme through the suppression of the immune system. Hardly conclusive proof of anything other than their inability to design a better trial.
You do know that they wouldn't have done the study right, if someone had already proven that these drugs work for 'chronic lyme'. Don't you? 😀
A lot of those comments are from butt-hurt Lymie quacks. In fact, they seem so upset - I might just choose this as a PhD topic to troll the **** out of as many of them as possible.
Tom, for all the bluster show, you're using one study that took 3 sample groups and treated them over 14 weeks. 3.5 months, using two antibiotics that have not and never have been proven to address persistent Lyme infection,
You'd think that they'd start with the drugs that are used to tackle acute lymes though? Wouldn't you, drugs that have been proven to work in neurological lymes disease eg doxycycline. 😀
a mean improvement in all test groups after the 14 weeks.
Oh you mean like in the placebo group as well?
and which doesn't mention patients possible coinfections with other tick-borne organisms such as Babesia or Bartonella, both of which impair the successful treatment of Lyme through the suppression of the immune system. Hardly conclusive proof of anything other than their inability to design a better trial.
I'm sorry, but I really don't think coinfections would statistically alter this study at all - there should be a representitive sample of coinfections in both the placebo group and the treatment groups - these coinfections do not intereact with antibiotics do they - you state that they intereact with the immune system.
A lot of those comments are from butt-hurt Lymie quacks. In fact, they seem so upset - I might just choose this as a PhD topic to troll the **** out of as many of them as possible.
Wow, and you say you want to get into unbiased medical research? You have managed some fairly harsh comments in this thread so far. It makes me hope you never persue a career in the actual health service or in policy making where being judgemental over people really isn't helpful or welcome.
No Mike, the public needs to get a grip and start listening to what medical researchers are saying - instead of issuing them with death threats because they spoke out against things like Morgellons etc. The lyme literate doctors are nothing more than Byzantine Alchemists who make money from preying on people.
Is this your new topic of experitse? I'm not claiming it's mine but you are often very quick to dismiss out of hand stuff. This does seem to be an area where understanding is poor and more data is needed.
The public will never listen to medical reseachers, they actually shouldn't as most are not euipped to do a full study of all available, on the other hand the medical researchers are often too close to topics to speak on the subject broardly. The body of research needs bringing together into public policy and it also needs highlighting where research has gaps/holes or not enough data.
Myabe you just need to chill a bit.
Ernie... Can I give more details?
Well, NOT really..it's a process that many ccgs are going through.
If you Google 'ccg decommissioning plans' there's a few who have published theirs..knock yourself out.
Stopping services (as opposed to reducing them via thresholds changes) is clearly a last ditch attempt to save money.
The reality is the nhs cannot afford it's current level of activity.
And there lies the crunch ,, the vast majority of overspend is increase in activity, rather than significant waste. More things are happening.
Three kids cost more than two.
Two cars cost more than one....
We need to sensibly reduce activity.
DrP
Tom_W1987 - Member
You do know that they wouldn't have done the study right, if someone had already proven that these drugs work for 'chronic lyme'. Don't you?
So you're now agreed that you can't make a blanket statement regarding the efficacy on longterm antibiotic treatment based on just two drugs, and that you're distinction between quacks and 'real science' also accommodates a considerable lack of knowledge in both parties? Excellent.
[b]A lot o[/b]f those comments are from butt-hurt Lymie quacks. In fact, they seem so upset - I might just choose this as a PhD topic to troll the **** out of as many of them as possible
Why not? You're ambition seems to be acting like a Phd level troll on here. Or you could do something medically useful. Either way, they raise pertinent and informed questions about the quality of that study and unlike you many have a Phd. Internet troll vs Doctor?
[b]You'd think[/b] that they'd start with the drugs that are used to tackle acute lymes though? Wouldn't you, drugs that have been proven to work in neurological lymes disease eg doxycycline.
you would, wouldn't you? And yet, they are already shown to have improperly used IV ceftriaxone by using it for less than the lifespan of the borellia and it ignores current research regarding persistent or chronic Borellia infection that actually discuss in vitro and in vivo antibiotic efficacy in-depth. That would have been a better place to start, wouldn't it? Or from your lofty position of achievement do these scientists not meet your standards?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3132871/#__ffn_sectitle
a mean improvement in all test groups after the 14 weeks.
Oh you mean like in the placebo group as well?
You mean the placebo group that was also given a two week course of ceftriaxone? It's not really a placebo group anymore is it? They should perhaps have considered that when designing the study... Did you even read the paper beyond the abstract or are you just trying to save face and regurgitating whatever suits your purpose?
I'm sorry, but I really [b]don't think[/b] coinfections would statistically alter this study at all - there [b]should be[/b] a representitive sample of coinfections in both the placebo group and the treatment groups - [b]these coinfections do not intereact with antibiotics do they - you state that they intereact with the immune system.[/b][.
Yes, and if the study relies on measuring the production of antibodies in response to the treatment but the patient is immunosuppressed they won't get an accurate finding, will they? Again, did you actually read it?
You talk of Byzantine quackery that's been allowed to form in the vacuum of knowledge around this illness, but you're just the opposite side of the same coin, as opinionated as outspoken and half as informed as you'd like to believe. As mentioned up thread, you clearly have no interest in impartiality nor any empathy for the people the medical profession is supposed to treat with compassion. If you're real point of upset is patients arguing with doctors then I'm afraid you just need to get over the fact that illness is a subjective experience and patients are the ones that know how they feel better than anyone else. You don't know how much you don't know but you might at least try and be less unpleasant.
meanigless graphs time?
(sorry nabbed from a brexit page)
[img]  [/img]
[/img]
its not about just money though
public health is now the 'responsibility' of local councils who have seen theire biggest cuts to funding ever
acute staffing crisis aside its a huge factor into why hospitals and GPs are in crisis
I think describing the current situation as “a humanitarian crisis” is a bit over the top. The bigger question is that the demands of targets on individual trusts are probably – choosing my words carefully – leading to gaming. Equally we are all meant to have abandoned all elective surgery but there are strong suspicions that certain trusts are not following this; still doing certain surgery because they make so much money.What we are seeing is a breakdown in the trust and cooperation between different parts of the NHS. So we have seen mental health almost withdrawing from the sustainability and transformation plan process. We have major acute hospitals trying to protect their pre-eminent position by being too important/big to work with others. We have clinical commissioning groups in denial about their total absence of any long-term future. We have NHS England shouting down the phone at hard-pressed managers. We have NHS Improvement texting chief executives on Saturday afternoons checking that they are on top of the situation and expecting them to be at work.
Not one of these actions is going to help a hard-pressed consultant with targets – or more critically the patient. Worse than that, the pressure from above is largely political because government ministers and MPs cannot accept the reality of the general slide to a service that doesn’t meet what the public expect.
DrP - Member....the vast majority of overspend is increase in activity, rather than significant waste.
You say that as if it's not a self-evident fact!
And I totally reject the sentiment behind this comment : [i]The reality is the nhs cannot afford it's current level of activity".[/i] It is completely disingenuous as it suggests that the only solution is to cut the level of service rather than increase funding.
Healthcare is [i]always[/i] affordable, it is just dependent on commitment and priority.
No one, certainly no successful politician, would argue that due to increased costs of food some of the population should be allowed to go hungry or just simply starve. Or that due to increased costs of housing some of the population should be allowed to become homeless or just simply die of hypothermia.
So I see no reason why health should be treated any different or accept the suggestion that due to increased costs of healthcare some of the population should be allowed to become ill or just simply die.
Food and shelter has been a basic human need for hundreds of thousands of years, no one would argue with that, so also has physical and mental well-being.
If we as a society can afford cars, televisions, cinemas, chocolate, etc, we can afford to treat sick people.
It has been proven that by far the most efficient cost-effective provision of healthcare is a nationalised universal non-profit driven service. Therefore it is not a case of 'we can't afford the NHS' but that we can't afford not to have the NHS.
.
BTW I wasn't sure if you were taking the piss DrP so I didn't comment too much on what appeared to be some of your ludicrous suggestions in your original post, but can you explain some of the thinking behind this :
3-change thresholds for proven treatments; you need to be in MORE pain for a knee replacement, your cataract needs to be really bad for an operation etc
How does that work since for example cataracts progressively deteriorate? Is the idea to put off cataract surgery for as long as possible in the hope that the sufferer might die before surgery (possibly as the result of walking out in front of a car which they hadn't seen) and therefore saving a few hundred pounds?
What do you think the total saving to the NHS of delaying cataract operations might come to?
Interesting graph, is it from a realiable source?
The population growth that came after the war are in retirement now so we should be looking at a reduction in the pension spend as they pass away over the next 10/15 years. Also, the current state pension isn't mean tested either.
Quarter of the total for welfare!?
jekkyl - MemberQuarter of the total for welfare!?
It's a hateful lie.
That (now infamous) pie-chart includes pensions for teachers, nurses, police, etc, ie. state employees.
Pensions actually make up more than half of the 25% attributed to 'welfare'. My dad's not on welfare, he's a retired teacher.
In other words, the budget for pensions is *****ing huge. That's the budgetary elephant in the room.
It is completely disingenuous as it suggests that the only solution is to cut the level of service rather than increase funding.
Not quite. Its suggests both which is what medical bodies are also saying.
The level of service is already rationed anyway. That's how scarce resources are allocated when the state is the monopoly supply and the service is free at the point of delivery.
Re pensions, I lost the link but read yesterday the percentage of the budget that was absorbed last year by pensions. Makes you think..... 😉
Mike, I'll say it one more time. The rate of cost increase in the NHS is double the rate of growth of the economy (and we have tye best growth in the G7). Cost growth exists in the NHS independent of whether the economy's growing or not. Health care costs are rising party as new technology/drugs costs more not less and the population is growing and ageing. Your point about a growing economy is exactly what the PM said at PMQ again today, the Tories are the party to devliver that is her point
People are asking why there cannot be a cross party effort to address this and it's a very good question. The answer is neither party wants to face the real problem.
We need a total rethink
This is from DrP I agree wholeheartedly
The reality is the nhs cannot afford it's current level of activity.
And there lies the crunch ,, the vast majority of overspend is increase in activity, rather than significant waste. More things are happening.Three kids cost more than two.
Two cars cost more than one....
We need to sensibly reduce activity.
teamhurtmore - Memberit is completely disingenuous as it suggests that the only solution is to cut the level of service rather than increase funding.Not quite.
Yes it is. Cutting the level of service rather than increasing the funding is one solution but it is [b][i]not[/i][/b] the only solution. This thread has half a dozen pages of suggestions which include what other savings could be achieved to increase NHS funding.
Thank you making my point Ernie. You have corrected yourself, thank you.
This thread has half a dozen pages of suggestions which include what other savings could be achieved to increase NHS funding.
Most (all ?) of them not even Labour Party policy. It's a fantasy list of suggestions supported by virtually no one.
Even Corbyn himself doesn't propose abolishing the Trident programme, just the missiles but keeping the new subs.
We need a totao rethink
We need proper intergration between state and private provsion
We need people to pay for more private health insurance
We need higher taxes to oay for increased state spending, we are one of the very few countries without VAT on food and we have a much lower level of VAT on energy bills than does the rest of Europe. We need to address tax avoidance by the gig economy and tech companies
The solutions are out there. They are what everyone else are doing.
and the population is growing and ageing.
partially, the population is getting older, and in the west we're very good at identifying/stabilising/treating chronic conditions rather than catching them early enough to cure them. But mostly we're getting chronic lifestyle illness that don't lend themselves to a trip to a hospital to be "cured". Often I see people taking pills to "stabilise" one condition that needs a couple of other pills to alleviate the worst of the side-effects of the first...We are, as a population not paying enough attention to our own well being.
IMO, FWIW, we need to have a more much interventionist view on people's health, we have a system that tries to treat people once they are ill, where we need to have a system that prevents people getting ill in the first place, which is largely a social rather than monetary change. (although the countries with the best health outcomes spend something like 11% of GDP on health care vs the 7-8% we spend.)
I'd scrap the idea of a massive "national" NHS and go to a much more nuanced regional system without the "one size fits all" mentality that pervades the current system to it's detriment. let a culture of "do what works" grow.
Even Corbyn himself doesn't propose abolishing the Trident programme, just the missiles but keeping the new subs.
crazy lefties. that'd be like making the decision to have an aircraft carrier without any planes...
Teamhurtmore - MemberThank you making my point Ernie. You have corrected yourself, thank you.
Posted 30 minutes ago
God you're pathetic.
Yes increase VAT on food and energy (heating). It's a regressive tax so a suitable compromise in order to continue our "**** the poor" theme.
Why thank you Ernie, you are too kind.
(SQ, VAT is a tax on consumption not income so by defintion it cannot be regressive. That aside, carry on...)
VAT is a tax on consumption not income so by defintion it cannot be regressive.
you do talk the most utter bobbins sometimes
Ernie - you seem to be coming across very angry, somewhat agitated. I think it's skewing your replies..
You challenge the statement "The reality is the nhs cannot afford it's current level of activity" as if that's incorrect?
That statement is made 'now' as a snapshot of 'now'. Hence, it IS correct!
Can you afford 4 ferraris? If you can, great, but if not, the statement "ernie lynch cannot afford 4 ferraris" is true.
Yes, you might win the Lotto tomorrow, hence is no longer true. But today, it's true.
And (unfortunately) there was no jest in my statement suggestions on how to manage the current NHS crisis.
In a was (a very 'mail headline way') you are correct - taking the cataract threshold example (which IS just a quick example i typed over breakfast or something) then yes - by increasing thresholds you reduce the number of operations required hence reduce the cost of said operation. Some people may need an operation at a later date, some people may die of other causes, some people may never deteriorate to NHS operation thresholds.
Of course, there is also an additional spend required by NOT doing operations i.e you increase knee op threshold, you save money on knee ops by doing less, but you spend more on teh analgesia budget and physio budget.
If the saving > the new spend, then it's a goer.
Anyway, I know your agenda, you won't be skewed, you're not as 'aware' as you like to think you are, so all is forgiven...
DrP
jambalaya, earlier on the thread I did agree with you that increased taxation is required. But I also said I would only find that agreeable if there was a more equitable distribution of wealth in the country. Increasing taxation on spending is going to affect the poorest most.
Big row in the French Parliament today about health spending, Socialist government getting a battering but fighting back. Politics is politics.
Sorry if truth/accuracy is uncomfortable nick
(I will contact the Alevel examining boards to alter their marking schemes as this is a regular question, on your behalf)
Dr, don't worry, Ernie likes to make things up about what you said in order to argue with you/himself. Nothing new there. Your comments on services are echoed across the profession.
DrP - MemberErnie - you seem to be coming across very angry, somewhat agitated.
Your diagnostic skills are poor doctor.
@slow maybe maybe not. We do need a proper discussion. IMO wealth inequality is primarily driven by globalisation as there is unending supply of ultra cheap labour. This is going to hit the middle income earners too as the supply of uktra cheap skilled labour inc in services is growing very rapidly. A big chunk of the very wealthy in London now and in the future are Chinese. Think about that.
For example. As far as I am concerned lack of funding for education meant I had to pay a higher price in direct costs than I would have had to pay in taxes to get the quality I was looking for.
Cut the 25% who go to A&E who aren't genuine emergencies and could have accessed health care from their doctor or via phone (NHS figures)
Would cure the problem overnight
Your diagnostic skills are poor doctor.
Hence why you can't beat face to face appointments.
It's not like anyone is suggesting email/text/skype consultation should be the norm, are they... 🙄
DrP
In terms of individual income and wealth, a regressive tax imposes a greater burden (relative to resources) on the poor than on the rich: there is an inverse relationship between the tax rate and the taxpayer's ability to pay, as measured by assets, consumption, or income.
Who has more disposable income, rich or poor?
Based upon the your first answer, who pays more on food or heating as a proportion of income?
Therefore, could VAT be considered regressive?
If you could answer these questions directly it would be much appreciated.
om_W1987 - MemberYou do know that they wouldn't have done the study right, if someone had already proven that these drugs work for 'chronic lyme'. Don't you?
So you're now agreed that you can't make a blanket statement regarding the efficacy on longterm antibiotic treatment based on just two drugs, and that you're distinction between quacks and 'real science' also accommodates a considerable lack of knowledge in both parties? Excellent.
A lot of those comments are from butt-hurt Lymie quacks. In fact, they seem so upset - I might just choose this as a PhD topic to troll the **** out of as many of them as possible
Why not? You're ambition seems to be acting like a Phd level troll on here. Or you could do something medically useful. Either way, they raise pertinent and informed questions about the quality of that study and unlike you many have a Phd. Internet troll vs Doctor?You'd think that they'd start with the drugs that are used to tackle acute lymes though? Wouldn't you, drugs that have been proven to work in neurological lymes disease eg doxycycline.
you would, wouldn't you? And yet, they are already shown to have improperly used IV ceftriaxone by using it for less than the lifespan of the borellia and it ignores current research regarding persistent or chronic Borellia infection that actually discuss in vitro and in vivo antibiotic efficacy in-depth. That would have been a better place to start, wouldn't it? Or from your lofty position of achievement do these scientists not meet your standards?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3132871/#__ffn_sectitle
a mean improvement in all test groups after the 14 weeks.
Oh you mean like in the placebo group as well?You mean the placebo group that was also given a two week course of ceftriaxone? It's not really a placebo group anymore is it? They should perhaps have considered that when designing the study... Did you even read the paper beyond the abstract or are you just trying to save face and regurgitating whatever suits your purpose?
I'm sorry, but I really don't think coinfections would statistically alter this study at all - there should be a representitive sample of coinfections in both the placebo group and the treatment groups - these coinfections do not intereact with antibiotics do they - you state that they intereact with the immune system.[.
Yes, and if the study relies on measuring the production of antibodies in response to the treatment but the patient is immunosuppressed they won't get an accurate finding, will they? Again, did you actually read it
1) You shouldn't recommend a treatment until there is evidence to prove that it works. So even if the studies havent been done, Lymies shouldn't be demanding access to these antibiotics.
2) Many of the "doctorz" raising questions in the comments section are actually raising non questions in an attempt to discredit the paper in the eyes of those that dont know any better.
3) This study relied on quality of life indicators, not immune markers.
4) A placebo group that were never treated would not have passed an ethics committee for fairly obvious reasons, its still a perfectly fine contol for the studies intended question.
5) Do you even science, bro?
6) I can't be ****ed to check the validity of the accusation that they didn't treat one arm of the study properly, at the moment, as Im typing from a phone. But like all the other "crticisms" I think it will end up being refutted quite easily.
DrP - MemberIt's not like anyone is suggesting email/text/skype consultation should be the norm, are they..
Sounds like a brilliant idea. How much would it save the NHS?
Sorry if truth/accuracy is uncomfortable nick
The most common definition of whether a particular tax is regressive is that it affects the poor more than rich, which by any measure, expert of text book, VAT very clearly does. I'm content that this is the most common definition of "Is VAT a regressive tax"
If that doesn't fit your view, it's your look out, not mine
I get what DrP is saying, in a very brutal way its the most pragmatic course of action. The question we have to ask ourselves is whether we want our health provision granted in such a manner.
Cut the 'Around 1 in 10 hospital outpatient appointments are missed every year in England' again NHS figures
10% improvement here
[url= https://www.google.co.uk/search?q=ccg+decommissioning&oq=ccg+decommissioning+&aqs=chrome..69i57j0l5.8143j0j9&sourceid=chrome&ie=UTF-8 ]It's not just DrP saying it...[/url]
DrP
Edit - [url= https://shropshire.gov.uk/committee-services/documents/s13151/8%20Decommissioning%20Disinvestment%20Interim%20Policy.pdf ]This[/url] is quite an informative procedure document.
Yes increase VAT on food and energy (heating). It's a regressive tax so a suitable compromise in order to continue our "**** the poor" theme.
Exactly. VAT should be removed from items not added. The poor are the most affected by VAT relative to their income. It should only exist on luxury items, i.e. not on most food and not on energy.
