Forum menu
This would suggest surgeries are quieter than normal even with vaccinations to do.
haha, feel free to come to my surgery and tell my doctors and nurses that they should feel grateful for the little work they're getting. Average list size for GP in the UK is about 8000 pts, there are about 7000 practices in the UK, Even if every one of the dead people are registered, that's 21-ish patients from each surgery, that's a drop in the ocean. Without really checking I think I've had that many new patient registrations this week already.
You continue to only look at this your way, other opinions are out there, some more realistic and considered than your frequent petulant outbursts. You consistently present your opinions as facts but refuse to yield your position when called out on their inaccuracies. You know what this behaviour resembles don’t you?
You are digging yourself a troll-shaped hole there. Every time someone shouts troll, I see a closed mind refusing to engage with something that doesn’t fit their narrative.
Are you aware that the time being vaccinated as you call it, is just the bit where they stick the needle in your arm? There is a whole lot of other work going on at the same time that you’re not party to.
Although both my brain cells are currently busy transmitting data to Mr Gates, yes I am aware of that. Are you aware that the admin etc around the consultations and treatments I listed as not having had would dwarf that? My point stands. My personal health care burden has been a fraction of what it would have been.
They’ve got quite a substantial backlog to get through, so no, the GPs and medical staff are not twiddling their thumbs waiting for punters to arrive
Did I say that? But what backlog would surgeries have? Much of the hospital backlog will not materialise either due to people dying or getting better.
What is this absenteeism you are referring to? Please provide some context
I mean staff off with Covid.
If surgeries are in fact busier than normal, then I would be very interested in learning why. Which is why I raised the issue in the first place. Logic suggests to me that demand must be down.
Why is that, nickc? Everyone I know is staying away from the NHS as much as possible.
Logic suggests to me that demand must be down.
You are making a huge assumption that your demands on the NHS in the last year are in some way representative for other people, therein lies your first error in "logic".
Much of the hospital backlog will not materialise either due to people dying or getting better.
Yes the 52yr old lady who needs a hip replacement has obviously died according to your view
Have you considered, even for just one moment, that in the last 13months people could have developed new problems but have been unable to get an appointment until recently. It's very hard to diagnose ulcers or lymphoma over the phone
You also need to consider the wider perspective, not every GP practice is like yours, not every NHS Trust is like yours. Your comments are reductive but we all know that this is not a simple issue nor are there simple solutions
Why is that, nickc? Everyone I know is staying away from the NHS as much as possible.
people are still sick, the vast array of "lifestyle" illnesses we generally treat (chronic manageable conditions like asthma and diabetes) still need to be managed Throw into the mix that counterintuitively it's probably easier to "see" a GP these days, we're mostly doing online telephone or video conferences with patients, so the barriers that normally keep folk away have been removed. You don't have to come to the surgery in worktime anymore, you're doctor will actually call you.
edited
Throw into the mix that counterintuitively it’s probably easier to “see” a GP these days, we’re mostly doing online telephone or video conferences with patients, so the barriers that normally keep folk away have been removed.
That’s an interesting point. I hadn’t thought of that.
Why is that, nickc? Everyone I know is staying away from the NHS as much as possible.
Well, everyone I know is using the NHS as much as before. It's just the method of delivering the service that changed a bit.
Wife still getting her checkups with the neuro consultant and physios. Parents still having cancer checks, biopsies, heart checkups. Friend took a tumble, ambulance called, all OK, checkup with doc the next day, I called about an ear infection that wouldn't clear...
You are making a huge assumption that your demands on the NHS in the last year are in some way representative for other people, therein lies your first error in “logic”.
There will be all the usual ailments needing GPs’ attention.
Less various infections that have been reduced due to social distancing etc.
Less me (and possibly others too) not going to the GP for minor stuff.
Less the dead (many of whom needed lots and lots of care).
Less STW members doing no gnar.
Plus vaccinations.
That, to me, spelt reduced demand.
But it turns out people phoning up with trivial stuff they couldn’t be bothered to queue for before is outweighing that. Which is a surprise, and quite shocking.
But it turns out people phoning up with trivial stuff they couldn’t be bothered to queue for before is outweighing that. Which is a surprise, and quite shocking.
That's because you've overlooked all the people who put off being treated over the last 12 months who are now feeling it's safe to get looked at.
That, to me, spelt reduced demand.
That sounds like pent up demand waiting to be released to me. The NHS is going to be busier than ever over the next year, in all services.
There will be all the usual ailments needing GPs’ attention.
Those folk with long term chroinic diseases haven't gone away in any significant numbers, or suddenly got better, a few have died, but that's normal as well.
Less various infections that have been reduced due to social distancing etc.
STD are still at about the same level there have been, and we still have to vaccinate children, pregnant mums etc
Less me (and possibly others too) not going to the GP for minor stuff.
Not that I can see. Most middle aged blokes* tend not to go to the GP anyway, but our routine patient load hasn't changed at all
Less the dead (many of whom needed lots and lots of care).
Already been said, as a per-practice number, it's not significant
Less STW members doing no gnar.
Doesn't account for as much A&E as you probably think, and at best; sports injury visits to A&E happen over just a couple of days, and are pretty straightforward anyway.
Plus vaccinations.
Yet to take effect, give it some time.
That, to me, spelt reduced demand.
Demand hasn't changed, will increase as the backlog of unresolved issues stars to really make it's presence felt, plus Long-COVID, plus I'm expecting a mini up-tick in mental health problems.
*I'm assuming you're a middle aged bloke, apologies if I'm wrong.
Won’t most of those coughs and colds and rashes and grazes and vague aches and pains have cleared up by now?
(Oops, crossed post. Thanks for the insight, Nickc.)
Is that what you think people use their GP for?
Well if you go with anything else they direct you to casualty🤷♂️
Seriously, though, there must be a fair proportion of trivial things?
Has anyone read the book, sorry meant a communication, from a Derbyshire GP Practice to all their patients? @nickc? any thoughts?
Edit: here's a corrected link:
https://www.pulsetoday.co.uk/views/in-full-gp-practices-16-page-letter-to-patients/
Throw into the mix that counterintuitively it’s probably easier to “see” a GP these days, we’re mostly doing online telephone or video conferences with patients,
This has certainly been my experience. From a practice that previously was almost impossible to get an appointment. Response times have been impressive and consultations meaningful - right up to prescriptions sent direct to our village pharmacy. Where a physical examination has been required, that has also happened following a phone call.
The NHS has adapted and adopted remarkably well in this regard. It won't be going back. Teams or Zoom on every phone, doctor calls for Video, close up phone photo of boil/wart/rash... This was the preserve of the few prepared to pay in London 18mo ago. Their business model was adopted almost overnight.
My experience too. Our surgery had already embraced Engage Consult and telephone triage, guaranteed nurse or doctor phone contact the same day. They've maintained this level of service throughout, with the addition of video consultancy, accepting pics of symptoms and so on. Will obviously vary.
Also add to their workload the impending tsunami of mental health issues ranging from minor to very serious due to Covid-19 (isolation, anxiety, stress, depression etc. etc.)
from a Derbyshire GP Practice
Thanks for the ink CG, that's a depressingly familiar picture
Seriously, though, there must be a fair proportion of trivial things?
Apologies, missed this. It's fair to say that there's a subset of patients who come repeatedly to the surgery with trivial things. Those people are still the same group of patients that they were pre-COVID, and they still take the same effort on our part to deal with them. Most folk don't want to come to the GP and will only do so for serious complaints that need attention.
Video conferencing does have a couple of knock-on effects, It's harder to end a consultation, and it's harder to stop pats talking about multiple problems, so patient interactions are longer, and more difficult.
This would suggest surgeries are quieter than normal even with vaccinations to do.
If I was this ignorant and out of touch with the subject I was banging on about, I'd be very embarrassed.
...but you have empathy and humility.
Just finished some referrals for the Diabetic Eye Screening Project service we have here in Manchester and it made me think of this thread. I've just looked a 9 patients that need referrals, 5 of which have followed the same trajectory New pts->joint pain(online docs appt) ->blood test (nurse appt)-> diabetes diagnosis -> referral, all in just 2 weeks, so that's 9 new patients joined the practice now all going to have to have monitoring. so, that's just today. also there 56 eye screen results back from DESP work through...so yeah, good thing we're not trying to do a mass vaccination programme on the side.
Diabetes in particular is going to create more demand for health services given the likelihood of developing it is apparently increased by Covid-19 infection. I suspect the same is true as people who suffered lung damage and heart damage from Covid-19 age. I susect we will actually have more people managing chronic conditions, and more frail people, because of Covid-19.
I think there will also be more lifestyle related problems. If we're being honest I think a lot of people have drank more booze, ate more junk food etc in the last year
A GP friend was saying that they only allow 1 patient (with carer/family member) at a time. Then the surgery has to be thoroughly cleaned after each visit.
Because these patients think they're the only ones (the waiting room is empty), they start pouring out all their troubles, taking double the time that the appointment would normally take. My friend is worn out by it all and thinking of taking some proper time off.
Another friend working in the nhs says she doesn't have time to go to the loo.
Clive Dix, departing leader of the vaccine task force says C19 will be gone from UK circulation by August.
Ok then. No wonder he’s departing.
Just had an email and text from NHS advising me to rebook my vaccination as its the AZ vaccine and I'm under 40.
Thing is, I turn 40 1 week after the first jab!
I'm thinking I should just carry on and get it. What would STW do? Yay to AZ, or ney to AZ?
If offered the choice, I would take the Pfizer vaccine. But I am old and had the AZ and had COVID.
With regards to gone by August. Maybe. The PHE have released their updated data on Variants of Concern. The Indian variant B.1.617.2 is now listed. There is an impressive replacement of the Uk variant B.1.1.7 that looks faster then its emergence. The report is here
Here's plot of that data (Fig 17) from my own analysis. Recall that the UK variant does not read the S-gene - hence S-Gene Target Failure (SGTF) is used as a proxy for the B.1.1.7 strain. You can see in this data that emergence of SGTF and decline is just shifted in time, likely after multiple founder effects from importation of new variants from South Africa and India. This is "microscope epidemiology". This level of granularity has never previously been available in real time - does it matter? I'm not so convinced, I think vaccines will continue to offer protection against morbidity, if not symptoms.
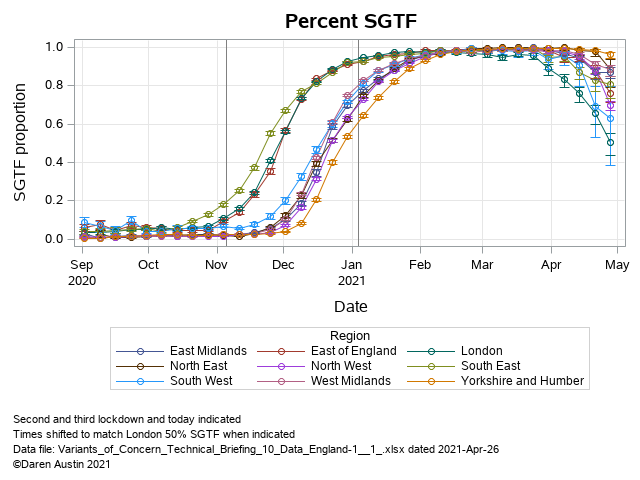
"SGTF" being ... ?
It's described above but I don't know what it is
S-Gene Target Failure - added in an edit. It's the proportion of Lighthouse lab Pillar 2 (community not hospital) tests that do NOT detect the spike protein (three genes are tested, Spike, Nucleocapsid and Open Reading Frame or orf). Used as a proxy for UK variant which is missing two amino acids in the spike protein at locations 69/70 and hence not picked up. The Indian, South Africa and wild type strains are S-gene target positive - hence the proportion of other strains is 1-SGTF. Hope that is clear?
Yes, thanks 🙂
Thanks for the link CG, that’s a depressingly familiar picture
Just as a follow on, you may be interested to read from the same place under "views" a piece by Copperfield that critiques the letter. Certainly food for thought imo.
Slight detour: under English regs, when can you have other people stay overnight in your house, if not in a bubble? Is it 17th May?
Is it 17th May?
I really hope so. I need to get home to see family 🙁
I think it is. We have the kids’ grandparents coming to stay straight away… they haven’t seen them for over 16 months. I’m mentally preparing for all the “how tall!” comments already.
Diabetes in particular is going to create more demand for health services given the likelihood of developing it is apparently increased by Covid-19 infection.
Hmm. Or the obese and overweight who have a much worse outcome from Covid are actually undiagnosed/pre-diabetic, and this is highlighted once they're in the system.
The GP surgery letter is interesting (if poorly judged for a surgery that wants to stay in business). My brother-in-law was a GP (died 2017) and had a term for this: sh!t life syndrome. Not a job I could ever do, for sure.
Things just keep getting grimmer in India - some back-of-the-envelope estimates of excess deaths in the tens of thousands per day. Truth is no-one will ever be able to find out the true figure.
https://twitter.com/ashishkjha/status/1391238136219512833
Christ that's grim reading
Horrendous in India, but no one over here takingbany notice as we can soon have little hugs.
My understanding was that India had quite a well developed bureaucracy as far as recording population went, even in the rural areas? Might be wrong, but we may get some accurately shocking data further down the line.
the numbers are horrific, a quick BOTE calculation says that for a population 20x the size of the UK, and we suffered 1300 deaths/day at our peak in January, 25-30K per day is not unlikely at all on a like/like basis. It's not that easy - different healthcare provision vs generally younger population, etc., but it's an indicator.
Other way - reporting 4000/day and scaling down to UK size that is 20/d which is us at end of April. Simply not credible, IMHO.
My understanding was that India had quite a well developed bureaucracy as far as recording population went, even in the rural areas? Might be wrong, but we may get some accurately shocking data further down the line.
Possibly, but I'm confident that it will be politically expedient to assign as few of those deaths to Covid as possible.
Horrendous in India, but no one over here takingbany notice as we can soon have little hugs.
That's a bit unfair, people have been through the wringer here as well. Folk can be forgiven for thinking of kith and kin
That’s a bit unfair, people have been through the wringer here as well. Folk can be forgiven for thinking of kith and kin
Yeah, sorry, my comment did not come across well. I was trying to say that the scale of the Indian crisis has been overtaken in UK media, even though it's got substantially worse and serves as a reminder that "we" are not properly protected until the world is protected.
Too late to amend my rather flippant sounding post now.
The problem I think seeing the disease in places like India is the scale of it is just mind boggling. The level of death is indescribable.
I read a tweet this morning of a woman in touch with a service desk to get help loading a product, and of course the service desk is in New Delhi, she says while they were waiting for the remote log on to load they made small talk, and he revealed that he'd lost a family member every week/10 days or so, there was just him and an uncle left...I can't imagine where to start with that.
Per capita mortality in the U.K. peaked at double the baseline rate. If one assumes the same across other countries, then one might see 20-25k deaths per day in India at peak. The U.K. has an older population and the over 85s were disproportionately hit. However the doubling was seen across all age groups consistently.
I imagine the reported 4000 is about 3-5 times lower than the true value, and the eventual collation of death certificates will show this. You can’t just hide the dead in a functioning democracy. Of course if 4000 was correct, then they are nowhere near the peak compared with other countries.
On the subject of my previous question a few pages back about returning to the gym:
RJ – my thoughts, please note these will not align with many posters in this thread:
the gym is legally open.
the risk of you ‘catching’ covid from gym eqpt which hasnt been sanitised to death is really really small.
the risk of you catching it in a packed spin class would be somewhat higher (but not because someone forgot to antibac your saddle and grips)
seems you are able to minimise your risk by visiting during quieter periods, cleaning your own equipment….. so thats positive.if you are concerned about taking it to your parents – stop seeing them till its all clear, or revisit your homegym cantbearseditis or a really difficult to manage scenario, dont visit your parents after going to the gym without some period of self observation/isolation.
I always went in quieter periods anyway, usually on the way home from visiting friends and family or sometimes in the middle of the night when I couldn't sleep! The plan is to now go on the way back from helping my parents out (maximum time between the gym and seeing them) and avoid the morning/evening rush as much as possible.
I’ve just started going back to my gym (Pure gym) and the cleanliness seems good. They’re doing a deep clean every night, and every piece of equipment gets cleaned down after every use by the user with anti bac wipes and pretty much everyone seemed to be doing this. Every other piece of equipment was closed off so you’re never that close to anyone else.
I messaged the gym's head office about my concerns and as a previous customer they offered me a free visit to chat to the staff about them (no training) which I did earlier today. The staff were perfectly open about it being a worry for them and that they've been very proactive on enforcing the rules on members. I asked why and the two I spoke to said straight that if they don't the place could be closed due to an outbreak and that's them both out of work. Can't argue with that mentality! So I've joined again and will see how it goes over the next few weeks.
I messaged the gym’s head office about my concerns and as a previous customer they offered me a free visit to chat to the staff about them (no training) which I did earlier today. The staff were perfectly open about it being a worry for them and that they’ve been very proactive on enforcing the rules on members. I asked why and the two I spoke to said straight that if they don’t the place could be closed due to an outbreak and that’s them both out of work. Can’t argue with that mentality! So I’ve joined again and will see how it goes over the next few weeks.
That's good to hear. Very fair of them to be that open and allow you a visit to see if you feel comfortable.
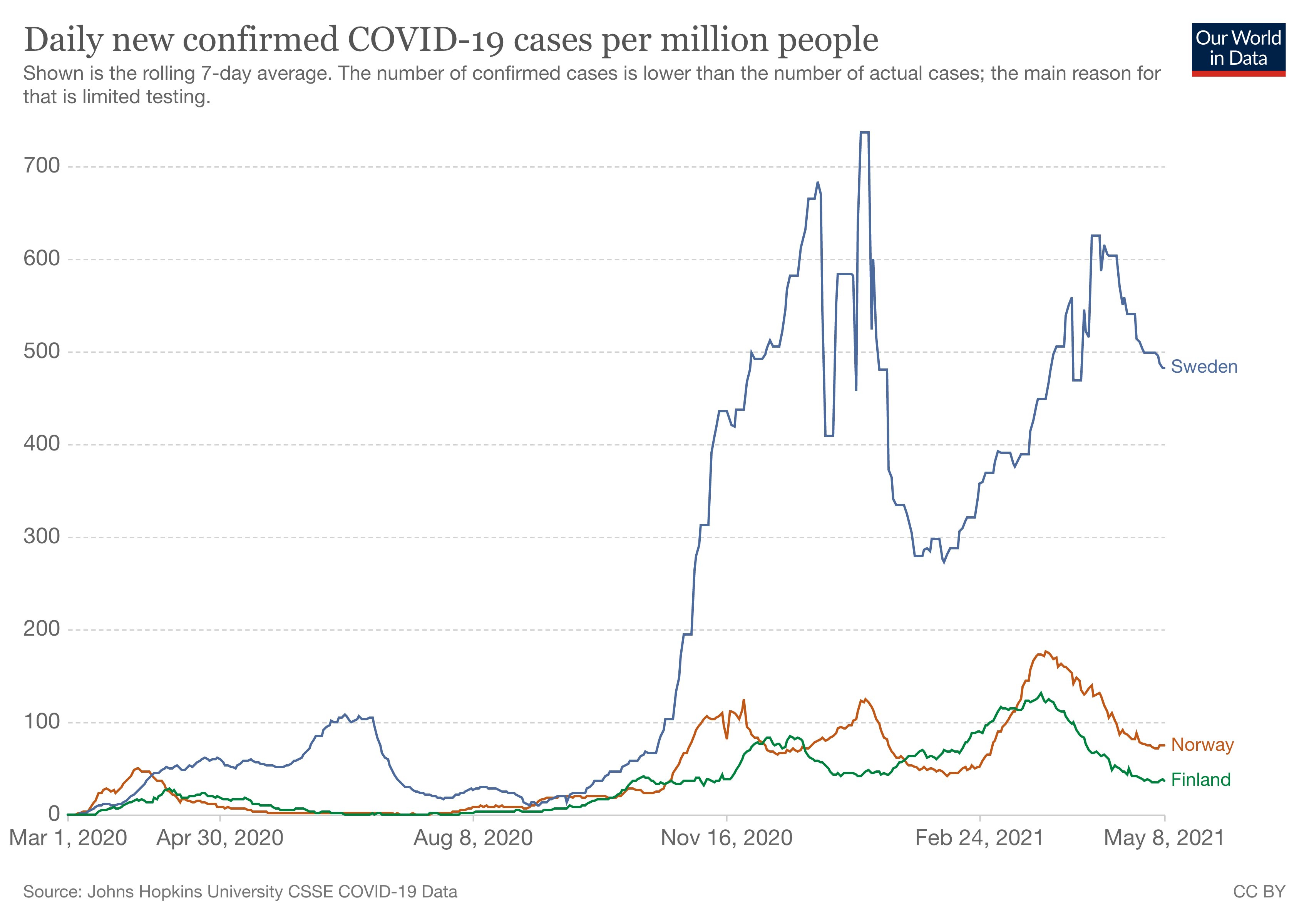
I know I've said that we'll possibly never know how well lockdown really works on an absolute scientific basis because there is no 'control' experiment
But for anyone claiming it doesn't because "Sweden", can we just declare that argument over now?
Other way – reporting 4000/day and scaling down to UK size that is 20/d which is us at end of April. Simply not credible, IMHO.
Agree - the 4k figure is, I assume, based on health care reported deaths. So the middle and upper class of the population, who can afford healthcare. There no mention of the lower class and unreported death toll - and seems to be an unwillingness in the media to investigate if the figures are different here.
@theotherjonv I'm certainly no anti-lockdowner, but as that's cases per 1 million, and we measure cases per 100,000 Sweden is sitting at about 47 per 100,000, not much more than the UK and we're well ahead in terms of vaccines.
Or have I got that completely wrong? (every chance!). 🙂
FWIW I'm very pro lockdown, for the simple reason we didn't really understand any other way to control early last year, and then we didn't really know how deadly/transmissable the Kent variant was, I don't think there was any other option.
Can you not add the UK to that chart, usually an option with OWID
Edit yes you can, but I'm failing to embed the image

That's showing UK at around 30 per million?. According to numbers I seen yesterday, then UK is ~22 per 100,000, so 220 per million?.
Or am I being dense? 🙂
@Nobeerinthefridge I think you're confusing new daily cases with something else. There were 15,327 new cases in the last 7 days ( https://coronavirus.data.gov.uk/) and UK population is about 67 million (Google), so about 15327/67/7 = 33 per million new cases as a 7 day average.
Aye, I get the maths, I think the per 100,000 is weekly new cases.
Let's compare UK and Sweden against not-UK and not-Sweden. Cases data from OWID site from today:
Spot the difference:
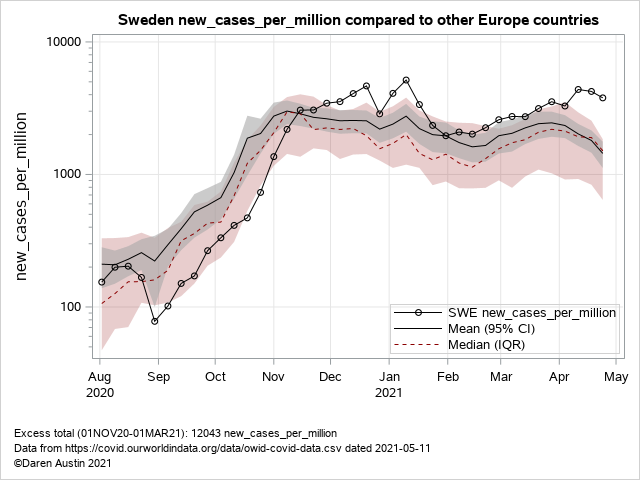
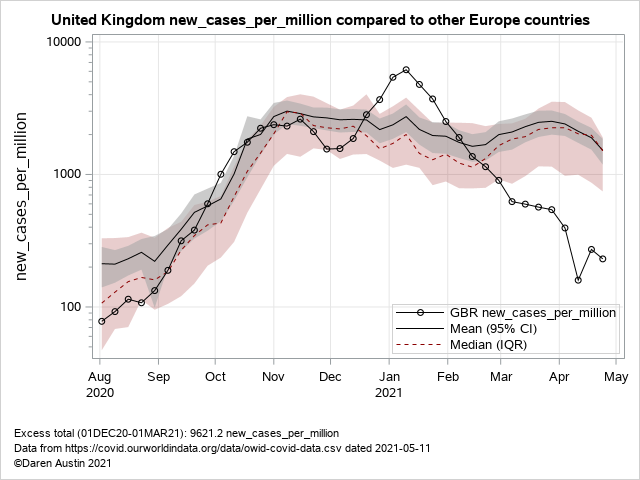
I think it's pretty clear that the UK is doing something right at the moment.
That's comforting to read.
Although the number of infections in Bolton have doubled in a week. Authorities urging people to have a test without symptoms. Let's hope in that area they can get on top of things.
Outbreak at that school has pushed Erewash to top of the national table apparently - we do need to stay cautious.
point of the graph I posted was that Sweden was frequently held up as having controlled their pandemic without strict lockdowns. Compare to its (culturally similar) neighbours, it seems they didn't.
As I say we can't truly know as you can't split a country in half and lock half down and let it run in another half. And you can't really compare different cultures / economic variable countries either. But SW vs FI and NO is not a bad guesstimate comparison.
TL:DR - lockdowns work. Vaccination works. Both together works very well......
I think it rules out the nonsensical seasonality arguments as well. The other countries look no better - as noted by the tight confidence interval and inter-quartile range. Lockdown and vaccinal immunity work.
at the moment.
we do need to stay cautious.
Let see where we are in June eh?
Outbreak at that school has pushed Erewash to top of the national table apparently – we do need to stay cautious.
What if I offered you a deal? We can "stay cautious" but also stop wearing masks in school classrooms and corridors. How does that sound?
https://www.bbc.co.uk/news/education-57059407
My 18 year old only has 3 more weeks before finishing college,but says he'd be happy to keep wearing a mask as he feels it's possibly helped reduce spread at the college - quite a few positive cases there since last September, small groups of friends having to isolate but no obvious in college spread, ie the contacts isolating don't appear to gave caught it
14 year old said last night - as we drove past said school - "what the heck are they doing for it to spread so fast?" Again, a few positive tests at her secondary school but again, no obvious in school transmission.
Fwiw, the academy with the outbreak is a new build and we wondered if the rapid spread may be due to their ventilation system maybe? Reports on the local news last night suggested that cases of the Indian variant in Nottingham are a cluster somewhere else and not the school as some had suggested
I can’t reconcile the removal of masks in schools for teens this term with keeping cases low enough to prevent emergence or spreading of new variants. Why not vaccinate teens over the summer break and stop mask wearing in September?
I can’t reconcile the removal of masks in schools for teens this term with keeping cases low
Schools are safe and have been since forever, remember?
We have (most) kids in school now, let’s keep ‘em there for the rest of term. Why risk sending more kids home again?
MCTD - you must be just round the corner from me.
I'm hoping the transmission between kids outside of school doesn't pass it on to the school where 2 of my kids are going through the exam chaos and the added stress that causes
Meanwhile in Sunny Spain Mrs DOD got a phone asking her to rock up at the local sports centre for a dose of moderna on Saturday.
Mines likely to be the following weekend.
So It appears my Murcia online vaccination registration worked and got us into the system as we are both private health non retirees not registered in the local health system.
Worth having your Facebook feeds following local news in Spanish as opposed to some of the ex-pat er groups.
Its not over yet:
Modelling by Imperial College's COVID-19 Response Team also found there could be a "small wave" of hospital admissions and around 9,000 additional deaths by June 2022 if steps three and four of the roadmap continue as scheduled.
They said the timing and size of a third wave will depend on the levels of transmission between 17 May, when restrictions are next eased, and 21 June, when all limits on social contact are due to be removed.
But, if variants of concern emerge that are comparable to the Kent variant, the third wave could be "substantially larger" - both in hospital admissions and deaths - than the spike in the winter of 2021, the researchers said.
Yikes.
And the link for that https://www.imperial.ac.uk/news/220894/latest-models-suggest-smaller-third-wave/
I thought a 3rd wave had already been forecast, even mentioned by Boris?
And why does 9000 excess deaths over the next 13 months seem optimistic?
So our quarantine period of two weeks is over and we all got tested today and are all negative which means we are allowed to rejoin society! In our case our 9yo son caught it from another boy in his class. We have since found out that seven other kids in his class tested positive and one educator. But of those eight only two showed any symptoms at all, my son and one of his best friends.Our son then infected the whole family at home (seven of us and the only ones to show symptoms were myself and Mrs Stern. Not sure if the first vaccine shot helped us or not We weren’t hospitalized!
MCTD – you must be just round the corner from me.
*Waves from Ilkeston *
Fully recovered RS?
What symptoms did you experience?
Which vaccine, how many shots, and when?
Unlocking papers are published today on the SAGE website here if interested.
Questions I am interested in; If no surge is noted, which part of the model is wrong? If a significant replacement of UK variant is noted, how does this change the model predictions?
Models only capture the current essence of what's known. They now are all very good at describing what has been seen, including past interventions. But the challenge is the known unknowns that are not in the models; baseline hospital-acquired infections, new strain emergence, waning immunity from vaccines... Quite a long list. But they are one way of trying to capture all that we know to date. And we know a lot more than a year ago. But three and six months in the future is still a long way off in prediction land!
Australia vaccination program continues at quite a pedestrian pace - mostly to do with availability.
Apparently they are starting to vaccinate the 40-49 cohort in the next week or two (me!), as they are expecting shipments of Pfizer to ramp-up - and these have be earmarked for the under 40s.
It will be interesting to see what the uptake in Australia is - people seem far less motivated here to get a jab, mostly to do with the low impact of covid.