- This topic has 502 replies, 107 voices, and was last updated 7 years ago by Flaperon.
-
What to cut to fund the NHS?
-
kerleyFree MemberPosted 7 years ago
Yes but the 80 year old has had 20 more years to liver and make the most of a healthy life. Or are you proposing that people have a limit of one or two major medical treatments in a life time however long that may be?
I haven’t proposed anything. You are the one proposing that only rich people can have some quality of life with an illness or that people should be killed!
I am happy with how it works now, access for all. Just needs more money because there are more people in an increasingly aging population.
Money is easy to get (increase tax to over 40% earners), just that nobody wants to do it.Yes you can make the service more efficient, yes you can cut other things but ultimately that won’t be enough so it needs more money.
Majority would be happy to pay more tax if it was all going direct to NHS. Or that’s what they say until it hit’s their wages…
jambalayaFree MemberPosted 7 years agoIndeed Cinnamon. Indeed..
Let us have a look at Pharmaceutical companies and what they are charging for ‘life saving’ drugs……
OK understood. Then stop buying them because it’s decided they are making too much profit ? How long do you think a Government could keep that up for ? Patients dying in UK whilst being treated in Ireland or Spain with “expensive” medicines.
chestercopperpotFree MemberPosted 7 years ago**** the poor. Am I right?
Seems to be the default answer regardless of whether it improves anything.
Oh dear the battlelines are drawn again too old **** off, too fat on your bike son, smoke yeah mate jog on, too rich do one. Yeah seems a recurring theme. We just need to get the list of exclusions right, preferably with more categories to please all the loonies 😀
Bring back hanging. What we need is a good war 😆
philxx1975Free MemberPosted 7 years agogood god 6 pages! what have I started.
Has anyone mentioned immigrants yet, or does that come in later at about page 10?
DrPFull MemberPosted 7 years agoThis is a very good question.
Really the answer comes in a few stages:
1- cut waste. Simple. Don’t prescribe when you shouldn’t, don’t double-pay providers of services. Don’t request needs you don’t use.
2-stop services without evidence our clinical benefit. This may be unnecessary or ‘little evidence’clinical treatments. Or services such as IVF.
3-change thresholds for proven treatments; you need to be in MORE pain for a knee replacement, your cataract needs to be really bad for an operation etc
4-reduce whole services -starting with those with the least impact.There you go.
Sorted.DrP
edit- it would be interesting for posters of the ideas above to consider what category they’d fit their suggestions into.
Not saying they are right or wrong, but makes you think…
Certainly over investigating and treating frail elderly would fall into category 2.Interestingly,i heard of a ccg that wouldn’t operate unless the patients gave up smoking. That’s a double win!
ernie_lynchFree MemberPosted 7 years ago4-reduce whole services -starting with those with the least impact.
Can you give more details? EG, start with those with the least impact and stop where?
BigEaredBikerFree MemberPosted 7 years ago1 – cut waste;
If the NHS was Walmart there is no way it would pay what it does for software licences, or IT consultancy rates. Collectively the NHS is massive and should really have the clout to dictate what it will pay. Instead (as I understand it) each trust negotiates it’s own purchases so lose the ability to collectively threaten to take all the business elsewhere if a vendors prices are not keen enough.
I know that prior to 2010 the NHS in England & Wales did have a half-decent agreement with one large software vendor. Then a new government talked about making cuts to save money and got rid of whatever department a previous government had established to manage these kinds of things.
So a saving of some centralised salaries meant that some NHS Trusts faced massive software licence fees (well in £ millions) when the old centrally negotiated agreements that previously covered them expired.
Speaking of software one of the key reasons the massive-super-expensive-project got so super-expensive was that the vendors were trying to please each hospitals requirements. They were not dealing with a single customer so no surprises it completely failed – I went to a fascinating seminar on that.
I’ve been told it’s not too dissimilar with how drugs are purchased and some are now a lot more expensive than in the past. I don’t know if true but certainly sounds plausible.
markrhFree MemberPosted 7 years agoHaven’t read all the posts so shoot me if some else has said this but, sell the houses of parliament off instead of rebuilding it (approx 5billion cost to rebuild) Find an empty office block (doesn’t really matter where, Its a connected world!) and move all muppets, sorry M.Ps and their staff out there and spend money saved, plus what we’d get for selling Westminster on NHS.
Its a start.ernie_lynchFree MemberPosted 7 years agoIt seems that you haven’t read the original post either 🙂
Get rid of Trident, would that be enough?
fergalFree MemberPosted 7 years agoOoops!!
Could anyone please give a rational justification for keeping Trident, i know brexiteers seem to think we are still some sort of imperial power, but really if it is just about job creation then at least be honest about it, rather than talk about unforseen threats.
PS. infact wholesale cuts to the military, why do we need such a large military anyway, i would like to see a defence force!
BigEaredBikerFree MemberPosted 7 years agoErm, numerically our military is pretty small. There’s not much left to cut if the government still wants to support international operations, and even then we have stepped back a lot in recent years whilst the focus has been on Afghan and Iraq.
The NHS and pension budgets also dwarf the defence budget. So yes it could help but given the way things work you soon be looking for something else and would have zero capability to do anything other than what the police and coastguard could manage.
Tom_W1987Free MemberPosted 7 years agoHi Tom,
again, we weren’t talking about climate change: you made the assertion that there is no proof that courses of antibiotics longer than current NHS pot-luck guidelines have any effect on Lyme, and that their supposed over-use by these patients diminishes the overall effectiveness of these medicines.
Here is a list of 700 peer reviewed medical papers that all support the claim that tick-borne diseases can persist and survive short term antibiotic use, all state the need for further research and large-scale sample groups: http://www.ilads.org/ilads_news/wp-content/uploads/2015/09/EvidenceofPersistence-V2.pdf
Please show me just one paper that states Lyme is comprehensively cured by a sub-30 day course of antibiotics, and can prove that longer term use is unnecessary. If you can’t do that, perhaps better to wind your neck in when talking about a subject you appear to know very little about. Just goes to show, all you need is one shit in the wrong woodpile and the whole house starts to stink.
Bwhahahahahahah.
None, I repeat none of those papers support the CLINICAL effectiveness of long term antibiotic therapy in humans. These studies have been done.
eg 1200 patients, well designed study, published in the New England Journal of Medicine?
http://www.nejm.org/doi/full/10.1056/NEJMoa1505425#t=article
Hmmmmm. Who do I believe, biased lobbying group or a study in the NEJM? A bunch of papers indirectly supporting a treatment and a good clinical trial?
fergalFree MemberPosted 7 years agoWell that is a myth, the fith largest spend in the world just behind Russia, having offensive capability has only made situations worse, Iraq, Afghanistan, libya are all operations that have caused a shit storm, destabilising the region has not helped.
IMHO we do not need to get involved in these foriegn adventures, if you are cutting public services you can not sustain a military that has historicaly been the backbone of an old imperial empire, something has to give.
jambalayaFree MemberPosted 7 years ago@fergel our military has been cut savagely over the past 30 years.
The Trident argument is a red herring imo. The Tories have promised to deliver an extra £10bn pa that’s double the Trident cost, yes “every bit helps” but Trident money isn’t going to transform the NHS/Health provision.
mikewsmithFree MemberPosted 7 years agoThe Tories have promised to deliver an extra £10bn pa that’s
Bollocks, Jamby the debunking of the 10bn has been shown multiple times. It’s like you and your 350 million it’s a crock of shit. Go find the report where it was said you had to manipulate the hell out of the data to get close. Saying it more doesn’t make it true, just makes you a liar.
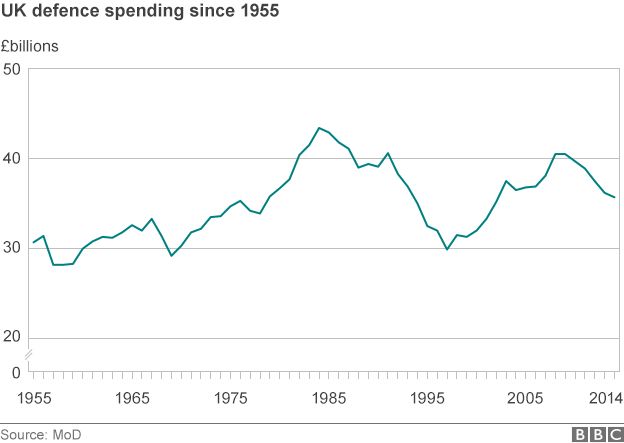
scotroutesFull MemberPosted 7 years agoAccording to my recent tax statement, the amount we spend on “defence” is around 26% of the amount we currently spend on health. Looks to me that we could redirect some of that spending.
jambalayaFree MemberPosted 7 years agoHealth Care spending (blue) and Defence spending (red). Up until 1987 we spent more on defence than the NHS.
 jambalayaFree MemberPosted 7 years ago
jambalayaFree MemberPosted 7 years ago@scotroutes Germany will be increasing defence spending by 80% to meet the NATO target.
mikewsmithFree MemberPosted 7 years agoSo do you accept that the 10bn figure is bollocks yet?
also nice graph, apat from the cost whats it telling me? Health Care spending is increasing. Nice to know, so long as the economy grows it’s a good thing.
As defence spending is also steadily increasing despite moving from a very expensive cold war into more peaceful times can the UK cope with the role it wishes to play in the world.Well that is a myth, the fith largest spend in the world just behind Russia, having offensive capability has only made situations worse, Iraq, Afghanistan, libya are all operations that have caused a shit storm, destabilising the region has not helped.
Is it having the capability or the way it went down made it worse? You can have the capacility and do some good with it, for instance sending a UN force of peace keepers to the Isreal/Palestine border to enforece some UN rules would be a very good thing.
jekkylFull MemberPosted 7 years agoGreat discussion, we really have a wealth of knowledge here. Some really interesting and insightful posts from people in the industry. The point from bigeared abdout IT and the fact that seperating the nhs into trusts, which was lauded as a progression to save money has actually ending up increasing costs. These are things which can be amended with correct governance.
What about in welfare, any cuts we can make there?
save pensions, pay people what they’re owed after paying in all their lives I reckon.ernie_lynchFree MemberPosted 7 years agoOoh, are we off posting meaningless graphs again?
Here’s mine – it’s from a BBC website :
And here’s another one also from the BBC
mikewsmithFree MemberPosted 7 years agoWhat about in welfare, any cuts we can make there?
save pensions, pay people what they’re owed after paying in all their lives I reckon.I think the consensus was a cull of other people. Back to the so long as I’m good, sure I must be taking more than I pay in mate.
NorthwindFull MemberPosted 7 years agojambalaya – Member
The Tories have promised to deliver an extra £10bn
What’s the exchange rate between a promised pound and a delivered one?
chompyFree MemberPosted 7 years agoTom_W1987 – Member
Hi Tom,
again, we weren’t talking about climate change: you made the assertion that there is no proof that courses of antibiotics longer than current NHS pot-luck guidelines have any effect on Lyme, and that their supposed over-use by these patients diminishes the overall effectiveness of these medicines.Here is a list of 700 peer reviewed medical papers that all support the claim that tick-borne diseases can persist and survive short term antibiotic use, all state the need for further research and large-scale sample groups: http://www.ilads.org/ilads_news/wp-content/uploads/2015/09/EvidenceofPersistence-V2.pdf
Please show me just one paper that states Lyme is comprehensively cured by a sub-30 day course of antibiotics, and can prove that longer term use is unnecessary. If you can’t do that, perhaps better to wind your neck in when talking about a subject you appear to know very little about. Just goes to show, all you need is one shit in the wrong woodpile and the whole house starts to stink.
Bwhahahahahahah.
None, I repeat none of those papers support the CLINICAL effectiveness of long term antibiotic therapy in humans. These studies have been done.
eg 1200 patients, well designed study, published in the New England Journal of Medicine?
http://www.nejm.org/doi/full/10.1056/NEJMoa1505425#t=article
Hmmmmm. Who do I believe, biased lobbying group or a study in the NEJM? A bunch of papers indirectly supporting a treatment and a good clinical trial?
Tom, for all the bluster show, you’re using one study that took 3 sample groups and treated them over 14 weeks. 3.5 months, using two antibiotics that have not and never have been proven to address persistent Lyme infection, and which doesn’t mention patients possible coinfections with other tick-borne organisms such as Babesia or Bartonella, both of which impair the successful treatment of Lyme through the suppression of the immune system. Hardly conclusive proof of anything other than their inability to design a better trial.
That paper is so flawed it would be like me taking three faulty washing machines and trying to fix them using a random assortment of tools used to fix lawnmowers then saying “I couldn’t do it in 30 minutes so they’re obviously broken” Can you imagine anyone saying “I couldn’t cure your HIV in 14 weeks with two drugs so sorry, there’s just no benefit to treating you further or doing any more research’? It demands money that isn’t being spent to establish why Lyme turns into a chronic illness in some people, and unfortunately there’s too many over-opinionated assholes like you that either don’t want or are unable to acknowledge the lack of science underpinning current policy and any emerging research that contradicts you.
If you cared to look at more recent articles on Lyme you’d see that even the man who designed current US Lyme treatment protocols admits he got it wrong on the bacteria being able to persist, and that their ability to alternate between blood-borne and cystic forms renders antibiotics between 60 to 1000 times less effective as a result. Does that mean long term antibiotic use is the solution? Perhaps not, but until actual research is done to establish what treatment is effective in chronic lyme cases then we won’t know, will we?
This article-published today-sums up the bias of arrogant tools like you quite well, but don’t let that stop you being a snarky **** whatever you do… Sincerely, my deepest hope for you is that you reap your own reward and get to deal with the kafkaesque process of being diagnosed and treated for Lyme-it might cultivate some humility alongside the bacteria.
chompyFree MemberPosted 7 years agoTom_W1987 – Member
Bwhahahahahahah.
Actually, if you care to read the comments on your own cited paper-from an assortment of scientists and doctors around the globe-they spell out quite clearly the flaws in the study, from the failure to account for the morphological nature of the bacteria, co-infections and also, that their own results showed that despite improper administration of IV antibiotics for a period shorter than the life of the bacteria, that there was… a mean improvement in all test groups after the 14 weeks. Too bad they attribute that to a placebo effect.
http://www.nejm.org/doi/full/10.1056/NEJMoa1505425#t=comments
.
Tom_W1987Free MemberPosted 7 years agoTom, for all the bluster show, you’re using one study that took 3 sample groups and treated them over 14 weeks. 3.5 months, using two antibiotics that have not and never have been proven to address persistent Lyme infection, and which doesn’t mention patients possible coinfections with other tick-borne organisms such as Babesia or Bartonella, both of which impair the successful treatment of Lyme through the suppression of the immune system. Hardly conclusive proof of anything other than their inability to design a better trial.
You do know that they wouldn’t have done the study right, if someone had already proven that these drugs work for ‘chronic lyme’. Don’t you? 😀
A lot of those comments are from butt-hurt Lymie quacks. In fact, they seem so upset – I might just choose this as a PhD topic to troll the **** out of as many of them as possible.
Tom, for all the bluster show, you’re using one study that took 3 sample groups and treated them over 14 weeks. 3.5 months, using two antibiotics that have not and never have been proven to address persistent Lyme infection,
You’d think that they’d start with the drugs that are used to tackle acute lymes though? Wouldn’t you, drugs that have been proven to work in neurological lymes disease eg doxycycline. 😀
a mean improvement in all test groups after the 14 weeks.
Oh you mean like in the placebo group as well?
and which doesn’t mention patients possible coinfections with other tick-borne organisms such as Babesia or Bartonella, both of which impair the successful treatment of Lyme through the suppression of the immune system. Hardly conclusive proof of anything other than their inability to design a better trial.
I’m sorry, but I really don’t think coinfections would statistically alter this study at all – there should be a representitive sample of coinfections in both the placebo group and the treatment groups – these coinfections do not intereact with antibiotics do they – you state that they intereact with the immune system.
mikewsmithFree MemberPosted 7 years agoA lot of those comments are from butt-hurt Lymie quacks. In fact, they seem so upset – I might just choose this as a PhD topic to troll the **** out of as many of them as possible.
Wow, and you say you want to get into unbiased medical research? You have managed some fairly harsh comments in this thread so far. It makes me hope you never persue a career in the actual health service or in policy making where being judgemental over people really isn’t helpful or welcome.
Tom_W1987Free MemberPosted 7 years agoNo Mike, the public needs to get a grip and start listening to what medical researchers are saying – instead of issuing them with death threats because they spoke out against things like Morgellons etc. The lyme literate doctors are nothing more than Byzantine Alchemists who make money from preying on people.
mikewsmithFree MemberPosted 7 years agoIs this your new topic of experitse? I’m not claiming it’s mine but you are often very quick to dismiss out of hand stuff. This does seem to be an area where understanding is poor and more data is needed.
The public will never listen to medical reseachers, they actually shouldn’t as most are not euipped to do a full study of all available, on the other hand the medical researchers are often too close to topics to speak on the subject broardly. The body of research needs bringing together into public policy and it also needs highlighting where research has gaps/holes or not enough data.Myabe you just need to chill a bit.
DrPFull MemberPosted 7 years agoErnie… Can I give more details?
Well, NOT really..it’s a process that many ccgs are going through.If you Google ‘ccg decommissioning plans’ there’s a few who have published theirs..knock yourself out.
Stopping services (as opposed to reducing them via thresholds changes) is clearly a last ditch attempt to save money.
The reality is the nhs cannot afford it’s current level of activity.
And there lies the crunch ,, the vast majority of overspend is increase in activity, rather than significant waste. More things are happening.Three kids cost more than two.
Two cars cost more than one….
We need to sensibly reduce activity.
DrP
chompyFree MemberPosted 7 years agoTom_W1987 – Member
You do know that they wouldn’t have done the study right, if someone had already proven that these drugs work for ‘chronic lyme’. Don’t you?
So you’re now agreed that you can’t make a blanket statement regarding the efficacy on longterm antibiotic treatment based on just two drugs, and that you’re distinction between quacks and ‘real science’ also accommodates a considerable lack of knowledge in both parties? Excellent.
A lot of those comments are from butt-hurt Lymie quacks. In fact, they seem so upset – I might just choose this as a PhD topic to troll the **** out of as many of them as possible
Why not? You’re ambition seems to be acting like a Phd level troll on here. Or you could do something medically useful. Either way, they raise pertinent and informed questions about the quality of that study and unlike you many have a Phd. Internet troll vs Doctor?
You’d think that they’d start with the drugs that are used to tackle acute lymes though? Wouldn’t you, drugs that have been proven to work in neurological lymes disease eg doxycycline.
you would, wouldn’t you? And yet, they are already shown to have improperly used IV ceftriaxone by using it for less than the lifespan of the borellia and it ignores current research regarding persistent or chronic Borellia infection that actually discuss in vitro and in vivo antibiotic efficacy in-depth. That would have been a better place to start, wouldn’t it? Or from your lofty position of achievement do these scientists not meet your standards?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3132871/#__ffn_sectitlea mean improvement in all test groups after the 14 weeks.
Oh you mean like in the placebo group as well?You mean the placebo group that was also given a two week course of ceftriaxone? It’s not really a placebo group anymore is it? They should perhaps have considered that when designing the study… Did you even read the paper beyond the abstract or are you just trying to save face and regurgitating whatever suits your purpose?
I’m sorry, but I really don’t think coinfections would statistically alter this study at all – there should be a representitive sample of coinfections in both the placebo group and the treatment groups – these coinfections do not intereact with antibiotics do they – you state that they intereact with the immune system.[.
Yes, and if the study relies on measuring the production of antibodies in response to the treatment but the patient is immunosuppressed they won’t get an accurate finding, will they? Again, did you actually read it?
You talk of Byzantine quackery that’s been allowed to form in the vacuum of knowledge around this illness, but you’re just the opposite side of the same coin, as opinionated as outspoken and half as informed as you’d like to believe. As mentioned up thread, you clearly have no interest in impartiality nor any empathy for the people the medical profession is supposed to treat with compassion. If you’re real point of upset is patients arguing with doctors then I’m afraid you just need to get over the fact that illness is a subjective experience and patients are the ones that know how they feel better than anyone else. You don’t know how much you don’t know but you might at least try and be less unpleasant.
kimbersFull MemberPosted 7 years agomeanigless graphs time?
(sorry nabbed from a brexit page)
its not about just money though
public health is now the ‘responsibility’ of local councils who have seen theire biggest cuts to funding ever
acute staffing crisis aside its a huge factor into why hospitals and GPs are in crisis
I think describing the current situation as “a humanitarian crisis” is a bit over the top. The bigger question is that the demands of targets on individual trusts are probably – choosing my words carefully – leading to gaming. Equally we are all meant to have abandoned all elective surgery but there are strong suspicions that certain trusts are not following this; still doing certain surgery because they make so much money.
What we are seeing is a breakdown in the trust and cooperation between different parts of the NHS. So we have seen mental health almost withdrawing from the sustainability and transformation plan process. We have major acute hospitals trying to protect their pre-eminent position by being too important/big to work with others. We have clinical commissioning groups in denial about their total absence of any long-term future. We have NHS England shouting down the phone at hard-pressed managers. We have NHS Improvement texting chief executives on Saturday afternoons checking that they are on top of the situation and expecting them to be at work.
Not one of these actions is going to help a hard-pressed consultant with targets – or more critically the patient. Worse than that, the pressure from above is largely political because government ministers and MPs cannot accept the reality of the general slide to a service that doesn’t meet what the public expect.
ernie_lynchFree MemberPosted 7 years agoDrP – Member
….the vast majority of overspend is increase in activity, rather than significant waste.
You say that as if it’s not a self-evident fact!
And I totally reject the sentiment behind this comment : The reality is the nhs cannot afford it’s current level of activity”. It is completely disingenuous as it suggests that the only solution is to cut the level of service rather than increase funding.
Healthcare is always affordable, it is just dependent on commitment and priority.
No one, certainly no successful politician, would argue that due to increased costs of food some of the population should be allowed to go hungry or just simply starve. Or that due to increased costs of housing some of the population should be allowed to become homeless or just simply die of hypothermia.
So I see no reason why health should be treated any different or accept the suggestion that due to increased costs of healthcare some of the population should be allowed to become ill or just simply die.
Food and shelter has been a basic human need for hundreds of thousands of years, no one would argue with that, so also has physical and mental well-being.
If we as a society can afford cars, televisions, cinemas, chocolate, etc, we can afford to treat sick people.
It has been proven that by far the most efficient cost-effective provision of healthcare is a nationalised universal non-profit driven service. Therefore it is not a case of ‘we can’t afford the NHS’ but that we can’t afford not to have the NHS.
.
BTW I wasn’t sure if you were taking the piss DrP so I didn’t comment too much on what appeared to be some of your ludicrous suggestions in your original post, but can you explain some of the thinking behind this :
3-change thresholds for proven treatments; you need to be in MORE pain for a knee replacement, your cataract needs to be really bad for an operation etc
How does that work since for example cataracts progressively deteriorate? Is the idea to put off cataract surgery for as long as possible in the hope that the sufferer might die before surgery (possibly as the result of walking out in front of a car which they hadn’t seen) and therefore saving a few hundred pounds?
What do you think the total saving to the NHS of delaying cataract operations might come to?



The topic ‘What to cut to fund the NHS?’ is closed to new replies.